Prevalence and Risk Factors of Cerebral Small Vessel Disease in a Chinese Population-Based Sample
Article information
Abstract
Background and Purpose
Epidemiological data of cerebral small vessel disease (CSVD) in the general population of China are lacking. We report on the prevalence of lacunes, white matter hyperintensity (WMH), and cerebral microbleeds (CMBs) in a community-based sample in China and compare the results with those of other studies.
Methods
This was a cross-sectional analysis of the population-based Shunyi Study in China. A total of 1,211 stroke-free participants (mean age, 55.6±9.3 years; 37.4% men) with available 3 Tesla (3T) magnetic resonance images were included in this analysis. Demographic information and risk factor data were assessed. The overall and age-specific prevalence of lacunes, WMH, and CMBs was evaluated. Associations between cardiovascular risk factors and the presence of these lesions were analyzed by multiple logistic regression.
Results
Our study showed a prevalence of 14.5% for lacunes, 72.1% for periventricular hyperintensity (PVH), 65.4% for deep white matter hyperintensity (DWMH), and 10.6% for CMBs. When compared with other community-based samples, individuals in the same age group showed a higher burden of lacunes and a relatively lower prevalence of CMBs. Advanced age was independently associated with the prevalence of these CSVD markers, while the presence of hypertension increased the risk of lacunes, PVH/DWMH, and CMBs in deep or infratentorial locations.
Conclusions
A higher burden of lacunes but a relatively lower prevalence of CMBs was observed in this Chinese population. This notable result highlights the challenge of CSVD prevention in China. Chinese have a risk factor profile for CSVD similar to those in other populations.
Introduction
Imaging markers of cerebral small vessel disease (CSVD), including lacunes, white matter hyperintensity (WMH), and cerebral microbleeds (CMBs) are commonly observed on brain magnetic resonance imaging (MRI) in elderly people. The reported prevalence of these lesions in elderly populations varies greatly across different studies, ranging from 8% to 33% for lacunes [1], 3% to 34% for CMBs [2,3], and 39% to 96% for WMH [4].
The epidemiology of stroke is variable across countries and ethnicities. Compared with White populations of European and US origin, Asians have been reported to have a two-times higher proportion of intracranial hemorrhage (ICH), and a different distribution of ischemic stroke subtypes [5,6]. In China, lacunar infarcts due to CSVD are thought to be responsible for a greater proportion of ischemic stroke than that in White populations [6]. In addition, CSVD, either due to hypertensive or amyloid vascular changes is the most important cause of ICH. One may infer from these data that CSVD may be more prevalent in Chinese stroke patients. However, studies investigating CSVD in the Chinese population are lacking, and whether there is a similar trend of CSVD in the general population as that in stroke patients is largely unknown.
On the other hand, the presence of CSVD not only increases the risk of subsequent stroke, but is also associated with cognitive impairment, motor and gait disturbances, urinary symptoms, and functional decline. Hence, investigating the population-based prevalence of CSVD in China is of great importance for healthcare services and research. Up to now, only one study of 321 individuals living in Shanghai has shown a higher prevalence of confluent WMH in Chinese (38.5%) than in Whites from Australia (28.4%) [7].
Given the lack of data, we performed a cross-sectional evaluation using 3 Tesla (3T) MRI to investigate the prevalence and risk factors of lacunes, WMH, and CMBs in a community-based Chinese sample. We further compared these data with population-based studies in other races.
Methods
Participants
Subjects were evaluated as part of a cross-sectional analysis (using baseline data at entry) of the Shunyi Study, an ongoing prospective community-based cohort designed to investigate the risk factors of cardiovascular and age-related diseases. All inhabitants aged 35 years or older living in five villages of Shunyi, a rural district nearby Beijing, were recruited. Between June 2013 and April 2016, a total of 1,594 individuals were enrolled (response rate, 71.3%). Standard clinical examinations were performed for each participant, including structured questionnaires, physical examination, and blood tests. In addition, all participants were asked to undergo brain MRI. Among these, 320 refused or had contraindications for MRI (cardiac pacemaker, coronary and peripheral artery stents, or claustrophobia), leaving 1,274 participants who underwent brain MRI. Compared with participants who underwent brain MRI, those who did not were older (59.4±12 years vs. 55.9±9.3 years, P<0.001) and more likely to be male (49.7% vs. 37.7%, P<0.001). For the present analysis, 63 subjects with a previous history of stroke were excluded, and a subsample consisting of 1,211 participants was used.
Each participant signed an informed consent form. All protocols of the study were approved by the Ethics Committee at Peking Union Medical College Hospital.
Demographic and cardiovascular risk factor assessment
We collected demographic and medical information, including age, sex, smoking status, body mass index (BMI), blood pressure, and presence of hypertension, diabetes mellitus, and hyperlipidemia. Blood pressure was measured three times and the mean value was used. Hypertension was defined as self-reported hypertension, treatment with antihypertensive medication, systolic blood pressure ≥140 mm Hg, or diastolic blood pressure ≥90 mm Hg. Diabetes mellitus was defined as self-reported diabetes, use of oral antidiabetic drugs or insulin, fasting serum glucose ≥7.0 mmol/L, or hemoglobin A1c (HbA1c) ≥6.5%. Hyperlipidemia was defined as fasting serum total cholesterol >5.2 mmol/L, low density lipoprotein cholesterol (LDL-C) >3.62 mmol/L, or use of lipid-lowering drugs. Smoking status was classified as current smoker (at least within the prior month) or non-current smoker. Venous blood samples, routinely drawn after an overnight fast, were analyzed for plasma total cholesterol, LDL-C, high density lipoprotein cholesterol (HDL-C), glucose, and HbA1c. Centralized blood assessments were used.
Brain MRI acquisition and analysis
MRI acquisition was performed using a single 3T Siemens Skyra scanner (Siemens, Erlangen, Germany). Three-dimensional (3D) T1-weighted images (T1WI) were acquired using magnetization-prepared rapid gradient-echo in sagittal planes (repetition time [TR]=2,530 ms, echo time [TE]=3.43 ms, inversion time [TI]=1,100 ms, field of view [FOV]=256×256 mm2, voxel size=1×1×1.3 mm3, flip angle=8°, 144 sagittal slices). T2-weighted images (TR=6,000 ms, TE=125 ms, FOV=230×230 mm2, flip angle=90°, slice thickness=5 mm, gap=1 mm, 80 axial slices), fluid-attenuated inversion recovery sequences (FLAIR; TR=8,500 ms, TE=81 ms, FOV=230×230 mm2, flip angle=150°, slice thickness=5 mm, gap=1 mm, 80 axial slices), and susceptibility-weighted images (SWIs; TR=27 ms, TE=20 ms, FOV= 208×230 mm2, flip angle=15°, slice thickness=1.5 mm) were acquired in axial planes.
MRI findings related to CSVD were classified according to standard published criteria [1,8,9]. Silent brain infarcts (SBIs) were defined as focal lesions 3 mm in size or larger, with the same signal characteristics as cerebrospinal fluid on all MRI sequences, and surrounded by a hyperintense rim on FLAIR images. We defined lacunes as focal deep infarcts 3 to 15 mm in size, mainly situated in basal ganglia or white matter. Both SBIs and lacunes were initially assessed on 3D-T1WI. Periventricular hyperintensity (PVH) and deep white matter hyperintensity (DWMH) were graded separately on FLAIR images according to the Fazekas scale. Fazekas scale ≥2 was regarded as severe PVH or severe DWMH. CMB was defined as a round or ovoid area of homogeneous signal loss on SWI, 2 to 10 mm in diameter with blooming effect. Anatomic localization of CMB was classified into three categories: lobar (cortical gray and subcortical or periventricular white matter), deep (deep gray matter: basal ganglia and thalamus, and white matter of the corpus callosum, and internal, external, and extreme capsules), and infratentorial (brainstem and cerebellum).
Three trained physicians who were blinded to clinical data rated lacunes, WMH, and CMBs, respectively. Each type of lesion was analyzed by a single reader (F.H. for lacunes and SBI, F.F.Z. for WMH, and Q.W. for CMB). Intrarater reliability was assessed on a random sample of 50 individuals with a 1-month interval between the first and second readings. Intrarater reliability expressed as kappa coefficient was as follows: 0.84 for Fazekas scale of PVH, 0.89 for DWMH, 0.95 for the presence of lacunes, and 0.90 for the presence of CMBs.
Statistical analysis
Descriptive statistics for the baseline demographic data and potential risk factors were presented. The crude prevalence of CSVD markers was plotted against 10-year strata. Age-standardized prevalence was calculated using the direct standardization approach with weights based on the World Health Organization world standard population for 2000 to 2025 [10]. Age-standardized prevalence of lacunes was compared with the 3C-Dijon Study [11], while that of CMBs was compared with the Rotterdam Scan Study [12] in specific age category.
Crude relationships of CSVD with age, sex, and vascular risk factors were assessed. We applied t-tests, analysis of variance, and the chi-square test to compare continuous and categorical variables between participants with and without each lesion type. Subsequently, a logistic regression model was constructed with odds ratio (OR) and 95% confidence interval (CI) to determine independent risk factors for each outcome. All analyses were initially adjusted for age, sex, and when appropriate, medication use. We then additionally adjusted for multiple variables, including current smoking status, BMI, hypertension, diabetes, LDL-C, and HDL-C.
Statistical significance was set at P<0.05 and all analyses were conducted using SPSS version 19.0 (IBM Co., Armonk, NY, USA).
Results
A total of 1,211 stroke-free participants were included in the present analysis. The mean±standard deviation (SD) age was 55.6±9.3 years, and 37.4% were men. The baseline characteristics of the study population are listed in Table 1. The prevalence of SBI, lacunes, WMH, and CMBs stratified according to 10-year categories are shown in Table 2.
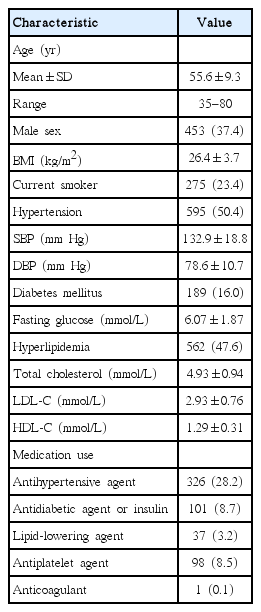
Baseline characteristics of the study population (n=1,211)
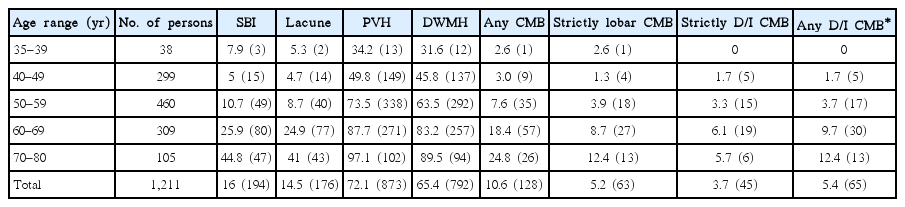
Age-specific prevalence of lacunes, white matter hyperintensity, and CMBs (10-year strata)
Lacunes
Overall, 194 participants (16%) had at least one SBI, of whom 176 (14.5%) had at least one lacune. The prevalence of lacunes increased with advancing age (P<0.001). Lacunes were more frequent in men (22.1%) than in women (10%). After adjustment for age and sex, the presence of lacunes was significantly associated with hypertension, higher systolic and diastolic blood pressure, and diabetes (Table 3). Hypertension (OR, 2.61; 95% CI, 1.71 to 3.97; P<0.001) and diabetes (OR, 2.15; 95% CI, 1.42 to 3.26; P<0.001) were independently associated with lacunes after additional adjustment for smoking, BMI, hypertension, diabetes, LDL-C, and HDL-C.

Association between vascular risk factors and lacunes, white matter hyperintensity, and CMBs in logistic regression models
White matter hyperintensity
The overall prevalence of PVH was 72.1%, and that of DWMH was 65.4%. Severe PVH and severe DWMH (Fazekas scale 2 and 3) were present in 18.2% and 10.5% of the subjects, respectively. WMH severity increased with older age in both brain locations (P<0.001). After adjustment for age and sex, both PVH and DWMH were significantly associated with hypertension and higher systolic blood pressure. Subjects with a higher level of serum fasting glucose had a higher risk of PVH (Table 3). After additional adjustment for smoking, BMI, hypertension, diabetes, LDL-C, and HDL-C, hypertension increased the risk of PVH (OR, 1.55; 95% CI, 1.15 to 2.09; P=0.005) and DWMH (OR, 1.51; 95% CI, 1.14 to 1.99; P=0.004), while no significant associations were observed between other vascular risk factors and WMH.
Cerebral microbleeds
Of subjects with CMBs (n=128, 10.6%), 53 (4.4%) had more than one. Microbleeds in a strictly lobar location were present in 63 subjects (5.2%). There were 65 persons (5.4%) who had microbleeds in a deep or infratentorial (D/I) brain region. Of these, 20 persons also had one or more lobar microbleeds simultaneously, while microbleeds in strictly D/I location were present in 45 subjects (3.7%). The prevalence of CMBs increased significantly with age for all locations (P<0.001). Male sex was related to the presence of any CMB and D/I CMBs (P<0.05), but not with strictly lobar CMBs. Age and sex-adjusted effects of cardiovascular determinants on the presence of CMBs are shown in Table 3. Hypertension, higher systolic and diastolic blood pressure, and lower LDL-C all increased the risk of D/I CMBs. No significant associations were observed between these risk factors and the presence of any CMB and strictly lobar CMBs. After multivariable adjustments of age, sex, BMI, smoking, hypertension, diabetes, LDL-C, and HDL-C, the above-described associations between hypertension, LDL-C and the presence of CMBs did not change.
Comparison of population based studies on prevalence of CSVD
In subjects aged 65 years or more, age standardized prevalence of lacunes in Shunyi Study is 37.2%, compared with 13.4% of the 3C-Dijon Study. In subjects aged 45 years or more, age standardized prevalence of CMBs in Shunyi Study was 12.7%, compared with 15.3% of the Rotterdam Scan study. The prevalence of lacunes and CMBs in specific age category are shown in the Supplementary Tables 1 and 2.
Discussion
In this community based, stroke-free Chinese cohort aged 35 to 80 years, our study showed a prevalence of 14.5% for lacunes, 72.1% for PVH, 65.4% for DWMH, and 10.6% for CMBs, which all increased with advancing age. Age and hypertension were the most common risk factors for CSVD.
With respect to ethnic differences, previous clinical studies performed in non-Asian countries have suggested that subcortical infarcts and confluent WMH are more common in non-Whites (e.g., Blacks, Hispanics, Asians) than in Whites [13]. Although ICH has been reported to be more prevalent in Asia, data on the prevalence of CMBs among different ethnicities remain limited. The estimated prevalence of lacunes in previous community-based studies varied from 8% to as high as 33% [1,2], and that of CMBs from 3% to 34% (Tables 4 and 5) [2,3,11,12,14-22]. Apart from the differences in age distributions, comparisons between population-based studies investigating the epidemiology of CSVD are further hampered in that the MRI scanning protocols, rating sequences, and diagnostic criteria are not uniform. 3C-Dijon Study, conducting in the European population, was similar to Shunyi Study in terms of rating sequences and diagnostic criteria for evaluating lacunes [11]. With regard to the same age ranges, the prevalence of lacunes in Shunyi cohort was higher than that of 3C-Dijon Study. Age standardized prevalence of lacunes in Shunyi Study was 37.2%, compared with 13.4% of the 3C-Dijon Study in subjects aged 65 years or more. This trend is also consistent with the higher prevalence of lacunes in other Asian studies shown in Table 4. The age standardized prevalence of CMBs in the Rotterdam Scan Study, which used a custom-made accelerated 3D T2* gradient-recalled echo (GRE) sequence, with sensitivity similar to that of SWI, was 15.3%, compared with 12.7% in the Shunyi Study [12].

Prevalence of lacunes in population-based studies

Prevalence of CMBs in population-based studies
In summary, when comparing participants in the same age group from Western world region, a higher burden of lacunes but a relatively lower prevalence of CMBs was observed in this Chinese population. Possible explanations for this discrepancy include the following. First, the higher prevalence of lacunes may be partly due to the higher burden of vascular risk factors and lower control rate in the Shunyi population, which relate to the low education and healthcare conditions in this typical rural sample in China. As listed in Table 1, the prevalence of hypertension was as high as 50.4%, whereas the rate of antihypertensive agent use was only 28.2%. By contrast, 43.2% of subjects in 3C-Dijon Study were taking antihypertensive agents. Since lacunes are associated with increased risk of subsequent stroke, cognitive impairment, and decline of daily living ability, more attention is needed to control vascular risk factors in the present population. On the other hand, we found it interesting that the higher burden of vascular risk factors and lower control rate did not equally contribute to a higher prevalence of CMBs in our cohort. Previous studies have demonstrated that antithrombotic therapy may increase the risk of CMB presence [22,23]. The very low proportion of subjects taking antiplatelet (8.5%) or anticoagulant (0.1%) agents may be an explanation. Second, Asians have been reported to have a higher likelihood of intracranial arterial stenosis as the cause of stroke compared with Whites [24]. The high prevalence of intracranial arterial stenosis in Shunyi Study (14% in stroke-free individuals, unpublished data, Yi-Cheng Zhu, 2017) may further contribute to the high prevalence of lacunes. Finally, genetic factors unique to Chinese ethnicity may be a possible explanation. Genetic studies have revealed that a non-synonymous single nucleotide polymorphism (rs2230500) in a member of the protein kinase C family, PRKCH (protein kinase C eta), had a significant association with silent infarction in Asians [25,26], while the minor allele is rarely found in European descendants. Therefore, genetic investigation is warranted in the Shunyi Study in order to determine why the prevalence of CSVD differed.
We demonstrated that increasing age was strongly associated with CSVD. Apart from age, hypertension is the most widely accepted risk factor in most studies. The current study replicated these findings. Blood pressure was associated with the presence of lacunes, PVH/DWMH, and D/I CMBs, reflecting their similar pathologies of hypertensive or atherosclerotic microangiopathy. We additionally confirmed that determinants of the presence of CMBs differed according to their location, which agrees with the viewpoint that CMBs in D/I locations are etiologically different from those that are strictly lobar in location.
The major strengths of our study are its population-based design, large sample size, and wide age range. Furthermore, 3D-T1WI and SWI were applied to evaluate lacunes and CMBs, respectively, with high resolution and sensitivity. There are still several potential limitations. First, subjects who refused to participate or those with MRI contraindications were generally older than individuals with available MRI data, leading to a possibility of selection bias. There were few participants in their thirties and eighties or older, resulting in poor estimation for these decades. Second, this study focused on the population in rural Beijing, which is a district in economic transition, with relatively higher prevalence but lower control rates of the vascular risk factors. These factors may limit generalizability of our conclusions to some extent. Third, we used a semiquantitative method to assess WMH. However, the intrarater reliability was excellent, and the visual rating is more clinically relevant than volumetric estimation.
Conclusions
In this community-based study of a Chinese rural population, we found a higher prevalence of lacunes, and a relatively lower prevalence of CMBs, compared with prior reports. The vascular risk factor profiles attributed to the burden of CSVD were found to be similar to those of other populations. In view of the very low awareness, treatment, and control rate of vascular risk factors in the present sample, health education for cardiovascular diseases in rural populations in China is a pressing issue. Whether genetic factors or undetermined environmental risk factors may play a role deserves further investigation.
Supplementary Material
Supplementary materials related to this article can be found online at https://doi.org/10.5853/jos.2017.02110.
Prevalence of lacunes in each age strata in Shunyi Study and 3C-Dijon Study
Prevalence of CMBs in each age strata in Shunyi Study and Rotterdam Scan Study
Notes
Disclosure
The authors have no financial conflicts of interest.
Acknowledgements
We acknowledge Pr. Christophe Tzourio and Aicha Soumare for their kind help in providing additional data of 3C-Dijon Study.
This study was supported by the National Key Research and Development Program of China (grant number: 2016YFC1300500505, 2016YFC0901004), the National Natural Science Foundation of China (grant number: 81173663), and National Key Technology R&D Program in the 12th 5-year Plan of China (grant number: 2012BAJ18B04-3, 2015AA020506).