Introduction
Critical blood pressure (BP) values in the acute ischemic stroke patients undergoing reperfusion treatment are based on the exclusion criteria in the pivotal Phase III trials of recombinant human tissue plasminogen activator (rtPA) [1,2]. These BP limits were applied in the most recent endovascular thrombectomy (EVT) studies [3]. However, there have been no randomized controlled trials specifically evaluating the proposed BP limits and there is uncertainty whether BP level of 185/105 mm Hg as an exclusionary criterion for reperfusion treatments can be generalized [4]. Notably, studies in hypertensive patients demonstrated a shift of the limits of functional cerebral blood flow autoregulation to higher values in patients with higher pre-stroke BP levels [5,6]. Thus, keeping BP at a certain universally defined level during the most vulnerable phase of acute cerebral ischemia seems counterintuitive. In animals models of stroke, cerebral blood flow in moderately under-perfused tissue depends on systemic BP and any significant drop in BP is likely to compromise penumbra viability [7]. However, BP beyond the proposed limits could be detrimental due to higher risk of post-reperfusion hemorrhages after EVT [8]. Oscillations in systolic blood pressure (SBP) after EVT may also be associated with poorer outcomes [9]. Earlier studies suggested U-shaped associations between on-admission BP and favorable clinical outcomes in ischemic stroke patients, but also poorer outcomes in patients with generally higher BP throughout hospitalizations [10-12]. One recent analysis reported an association between higher maximum in-procedure SBP and poor 30-day outcomes, while several others suggested the opposite—associations between poorer outcomes and indicators of BP dips [13-16]. Thus, we hypothesized that during EVT it would be reasonable to target individualized BP values. We therefore investigated the relationship between in-procedure SBP and mean arterial pressure (MAP) excursions to above or below the limits defined in respect to their pre-procedure values and (1) post-procedure imaging findings: ischemic lesion volume (ILV) and visible hemorrhages; (2) 3-month functional outcomes; in a cohort of adults with anterior circulation ischemic stroke treated with EVT.
Methods
Design
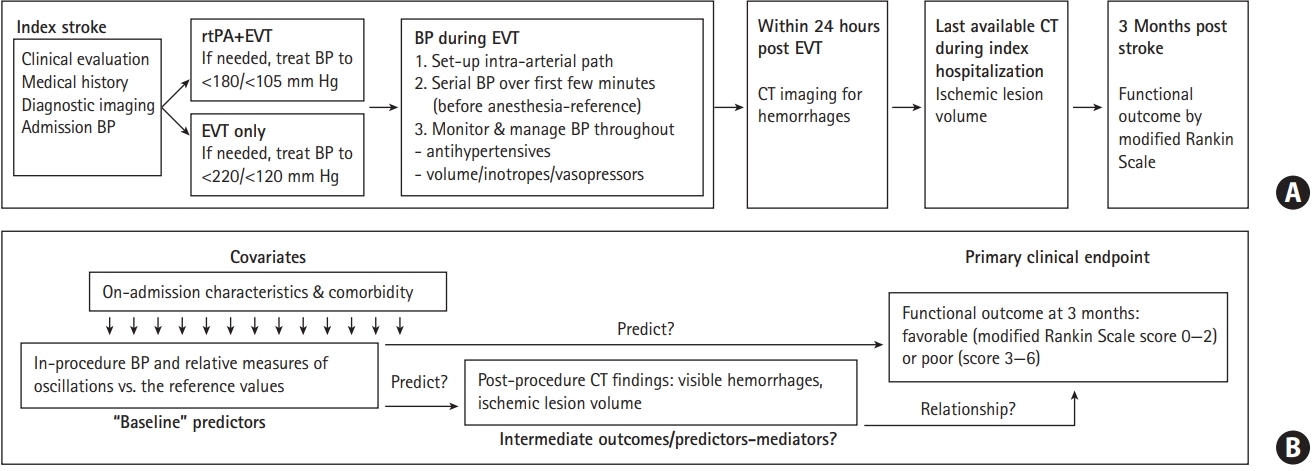
This is a retrospective analysis of a single-center prospective database comprising adults (age ≥18 years) with a symptomatic acute ischemic stroke due to occlusion of the internal carotid artery and/or middle cerebral artery treated with EVT using modern stent retrievers (a few patients received thrombus aspiration only) over a 5-year period (January 1, 2012 to December 31, 2016). It was approved by the Ethics Committee of Bundesland Salzburg. Figure 1A depicts the flow: patients underwent EVT under general anesthesia (GA) with or without intravenous rtPA, which individually required measures for BP reduction [4]; the analysis was restricted to patients with invasive BP measurement; serial BP values taken immediately before the start of EVT/induction of anesthesia were considered a “reference BP” for the period of the procedure; patients underwent post-procedure computed tomography (CT) imaging to assess hemorrhages and ILV, and were evaluated for the functional outcome at 3 months post-stroke (modified Rankin Scale [mRS]). We explored the associations between in-procedure BP oscillations defined in relative terms versus the “reference value” and (1) post-procedure ILV and visible hemorrhages; (2) favorable 3-month functional outcome (mRS 0-2) (Figure 1B).
Clinical evaluations
Stroke severity was assessed using the National Institutes of Health Stroke Scale (NIHSS). Indication for EVT was made in line with continuously updated standards, while indication for rtPA was in accordance with the Safe Implementation of Thrombolysis in Stroke-Monitoring Study [2,17]. At discharge, stroke etiology was classified according to the Trial of Org 10172 in Acute Stroke Treatment (TOAST) criteria [18]. Functional outcome at 3 months was assessed at scheduled visits or by a telephone interview with the patient or a proxy.
Radiological evaluations
CT or magnetic resonance was used to identify the vessel(s) portions occluded and to evaluate leptomeningeal collaterals on CT-angiography. Collaterals were graded as good when ≥50% were present as compared to the unaffected side. Postprocedure CT was used to evaluate presence of hemorrhages and last available CT during the index hospitalization to determine ILV [19]. The reperfusion success was graded by the Thrombolysis in Cerebral Infarction (TICI) scale: grades 2b (perfusion >50% of the vascular distribution of the occluded artery) and 3 (full perfusion with filling of all distal branches) were considered a success, grades 0-2a were considered a failure [20].
BP measurements and management
During EVT, BP was measured invasively every minute (except in two patients: every 2 or 5 minutes) and recordings were saved by the MetaVisionⓇ software (iMDsoft, Düsseldorf, Germany). Otherwise, it was measured regularly (cuff technique) and recorded in the patient charts. The in-house algorithm for acute stroke patients has been constantly in agreement with the respective guidelines, particularly in respect to the use of rtPA and EVT.
BP indicators
We determined the following BP indicators: (1) “reference” SBP/MAP as the mean of 3 to 5 measurements taken immediately before the start of EVT (induction of anesthesia); (2) individual values ±20% of the reference were determined and number of in-procedure excursions to values >120% or to <80% of the reference was counted to calculate their rates (episodes/10 minutes); (3) weighted mean in-procedure SBP/MAP by dividing area under the curve of BP over time (first to last in-procedure measurement) by the time period covered. We also determined rates of any excursions exceeding ±20% of the reference, and absolute (by linear interpolation) and relative (percent) time of the procedure with SBP/MAP >120% or <80% of the reference values.
Data analysis
We first evaluated associations of in-procedure BP with postprocedure ILV and hemorrhages, and then with 3-month mRS 0-2 (Figure 1B). General linear models were fitted to ln-transformed ILV (effects are geometric mean ratio [GMR], exponents of coefficient obtained with logarithms) and logistic models were fitted to hemorrhages and mRS 0-2. We considered rates of excursions to >120% and to <80% of the reference (analyzed jointly due to potential off-setting effects) to be the primary indicators of BP oscillations, as they were determined directly. Analyses based on derived indicators (absolute/relative time) provided virtually identical results, and are not shown. Analyses of the rate of any excursions exceeding ±20% provided no additional information (also not shown).
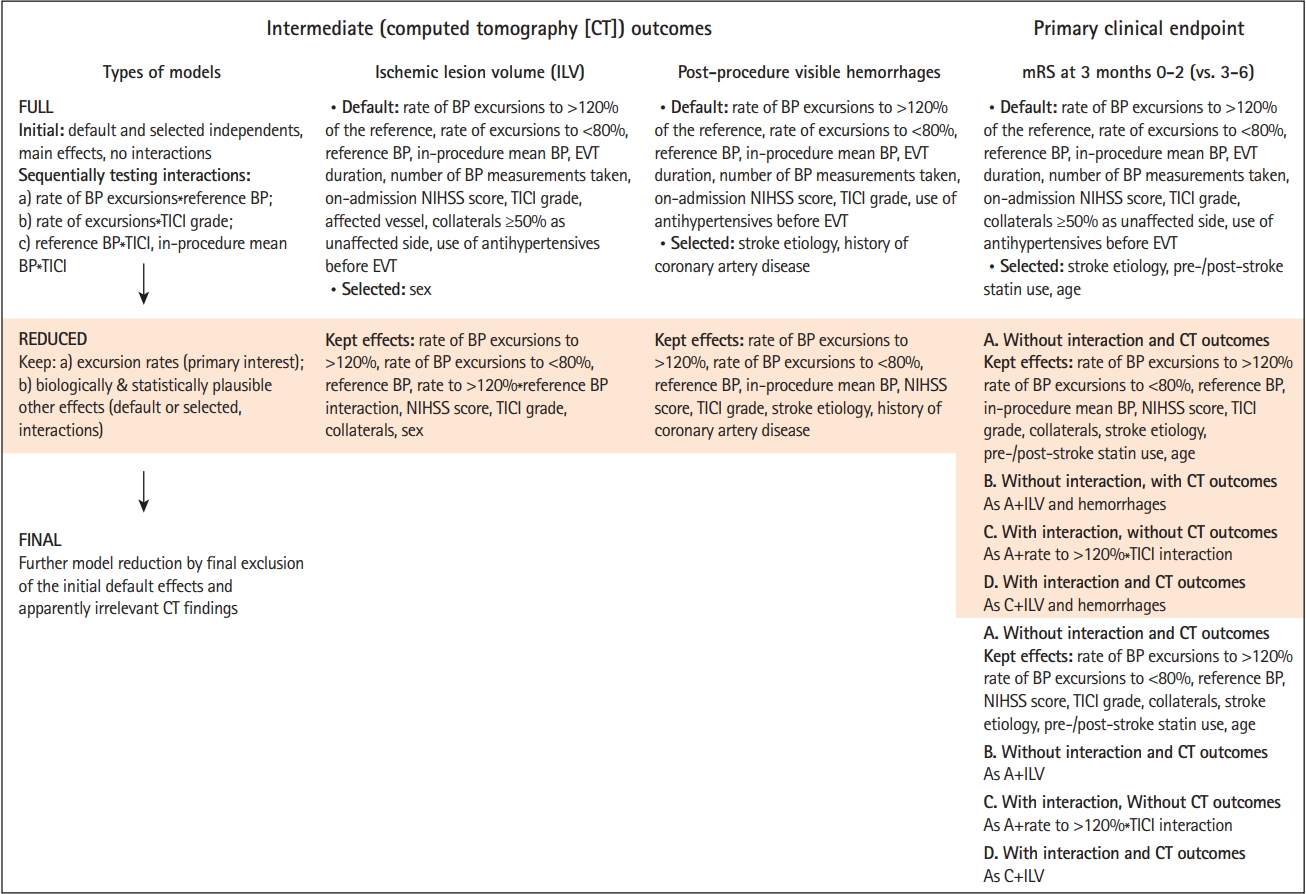
Several models were fitted to each outcome starting with larger (“full”) models (default and selected effects [stepwise selection with P<0.200 to enter/stay] with sequential tests of interactions: excursion rates*reference BP, excursion rates*TICI grade, reference BP/in-procedure mean BP*TICI grade), from which “reduced” models (to avoid overfitting) were derived (effects of primary interest and biologically/statistically plausible adjustments). In the analysis of 3-month mRS, intermediate outcomes (ILV, hemorrhages) were introduced as adjustments into the “reduced” models, so model selection included a further step to “final” models. Figure 2 outlines the model selection procedure. For details on multivariate model building and selection see Supplementary Methods. Mediation analysis [21] evaluated possibility that the effects of BP on the functional outcome were mediated “through” the effects on ILV/hemorrhages. We used SAS version 9.4 statistical software (SAS Inc., Cary, NC, USA).
Results
Patients
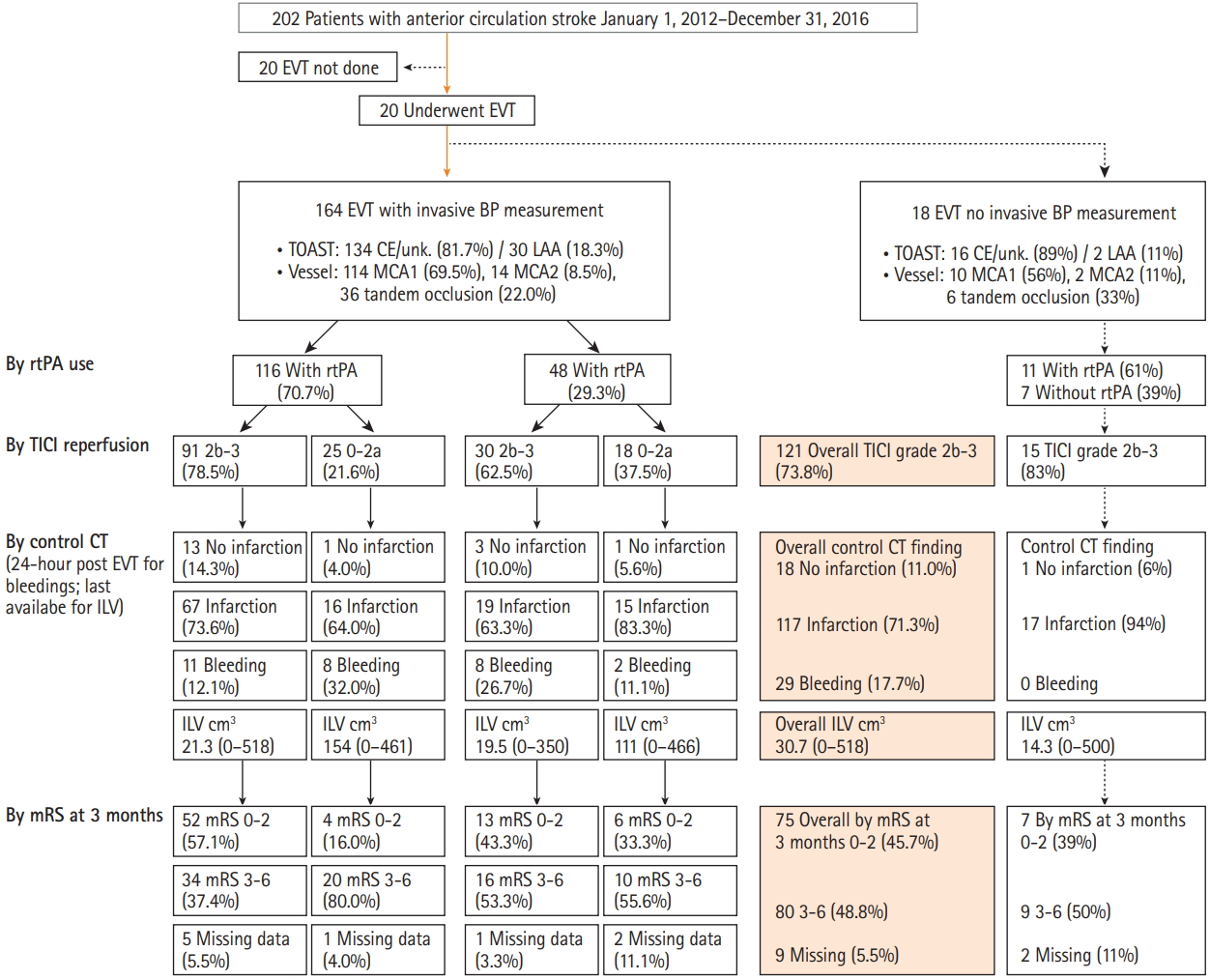
Of the 202 admitted patients, 20 did not undergo EVT and 18 did not have invasive BP monitoring. The cohort analyzed for ILV and hemorrhages comprised 164 patients, while 155 were analyzed for 3-month mRS (nine patients lacked data) (Figure 3).
Patient characteristics are summarized in Table 1 (Supplementary Table 1 for laboratory tests). Both on-admission and reference SBP/MAP varied greatly. Reference values appeared considerably lower than on-admission values, although intraindividual differences extended from substantial reduction to a substantial increase (Table 1). A total of 16 patients received antihypertensives between admission and EVT and two received sympathomimetics. Procedure lasted 12 to 587 minutes with 13 to 230 BP measurements, and 77 (46.9%) patients received sympathomimetics during EVT (Table 1). Overall, 38/164 (23.2%) patients had no excursions exceeding ±20% of the reference SBP/MAP, 68 and 70 (41.5% and 43.6% for SBP and MAP, respectively) experienced exclusively excursions to >120%, 37 and 31 (22.6% and 18.9%) exclusively excursions to <80%, and 21 and 25 (12.8% and 15.2%) experienced both. Data are summarized in Table 1 (see also Supplementary Table 2 and Supplementary Figure 1; for absolute/relative time >120% and <80% of the reference). Additional BP analysis (Supplementary Analysis of Blood Pressure) indicated that BPrelated procedures were guided by the intention to keep BP within the recommended limits, and not by the presenting stroke characteristics.
Relationship between in-procedure BP and ILV/post-procedure hemorrhages
Of the 164 patients, 132 (80.5%) had good collaterals, 121 (73.8%) achieved successful reperfusion, ILV ranged 0 to 518 cm3 and 29 (17.7%) patients had visible hemorrhages (Table 1). Full models were fitted to each outcome (see Supplementary Tables 3 and 4 for complete models). Independent variables consistently not associated with the outcomes were consecutively removed (Figure 2). Reduced models are shown in Table 2. Higher rate of in-procedure SBP excursions to >120% of the reference was associated with lower ILV, more so at higher reference values (rate*reference interaction) (Table 2). As an illustration, with reference SBP <120 mm Hg (n=62) the adjusted GMR=0.89 (interquartile range [IQR], 0.74 to 1.08), with reference SBP >135 mm Hg (n=60), GMR=0.34 (IQR, 0.15 to 0.74). The effect of SBP excursions was consistent in patients with TICI 0-2a (n=43) and TICI 2b-3 (n=121) (Supplementary Table 3). SBP excursions to <80% of the reference were not associated with ILV. Higher admission NIHSS score and male sex were associated with higher ILV; TICI grade 2b-3 and good collaterals were associated with lower ILV. Similar associations were observed for MAP, except for the excursions*reference interaction (Table 2).
In-procedure BP oscillations assessed by BP excursions were not associated with the post-procedure hemorrhages, higher reference SBP/MAP tended towards higher odds, while higher in-procedure mean SBP/MAP was associated with lower odds of hemorrhages (Table 2 and Supplementary Table 4). Higher in-procedure SBP/MAP was determined mainly by the higher reference SBP/MAP (Supplementary Analysis of Blood Pressure, Table F). Further analysis demonstrated that higher reference SBP/MAP was indirectly (via in-procedure mean) associated with lower odds of post-procedure hemorrhages: the indirect effect was practically identical in size to the direct effect (Table 2); hence, the total effect was close to zero (Supplementary Analysis of Post-Procedure Hemorrhages).
Relationship between in-procedure BP and 3-month functional outcome
Patients with mRS 0-2 (75/155, 48.4%) appeared younger, were more commonly men, and less commonly suffered comorbidities than the patients with mRS 3-6 (Table 1). They were more frequently pre-index stroke statin users, and less frequently antiplatelets or anticoagulants users (Table 1). On-admission NIHSS score, prevalence of cardioemobolic/unknown etiology and of tandem occlusions were lower while the use of rtPA was more common and the onset-to-EVT time was shorter in patients with mRS 0-2 (Table 1). Average on-admission and reference SBP/MAP appeared similar between the two subsets and similarly low numbers of patients received antihypertensives between admission and EVT. BP decline between admission and EVT appeared somewhat greater in patients with mRS 3-6 (Table 1). Weighted mean in-procedure SPB/MAP appeared comparable, while rates of excursions to >120% or to <80% of the reference appeared higher in patients with mRS 0-2. Similar proportions of patients received sympathomimetics during EVT (Table 1). Patients with mRS 0-2 more frequently had good collaterals, were more frequently successfully reperfused, their ILV was lower and visible hemorrhages were less frequent. They were less frequently post-stroke statin users, likely due to confounding by indication (Table 1).
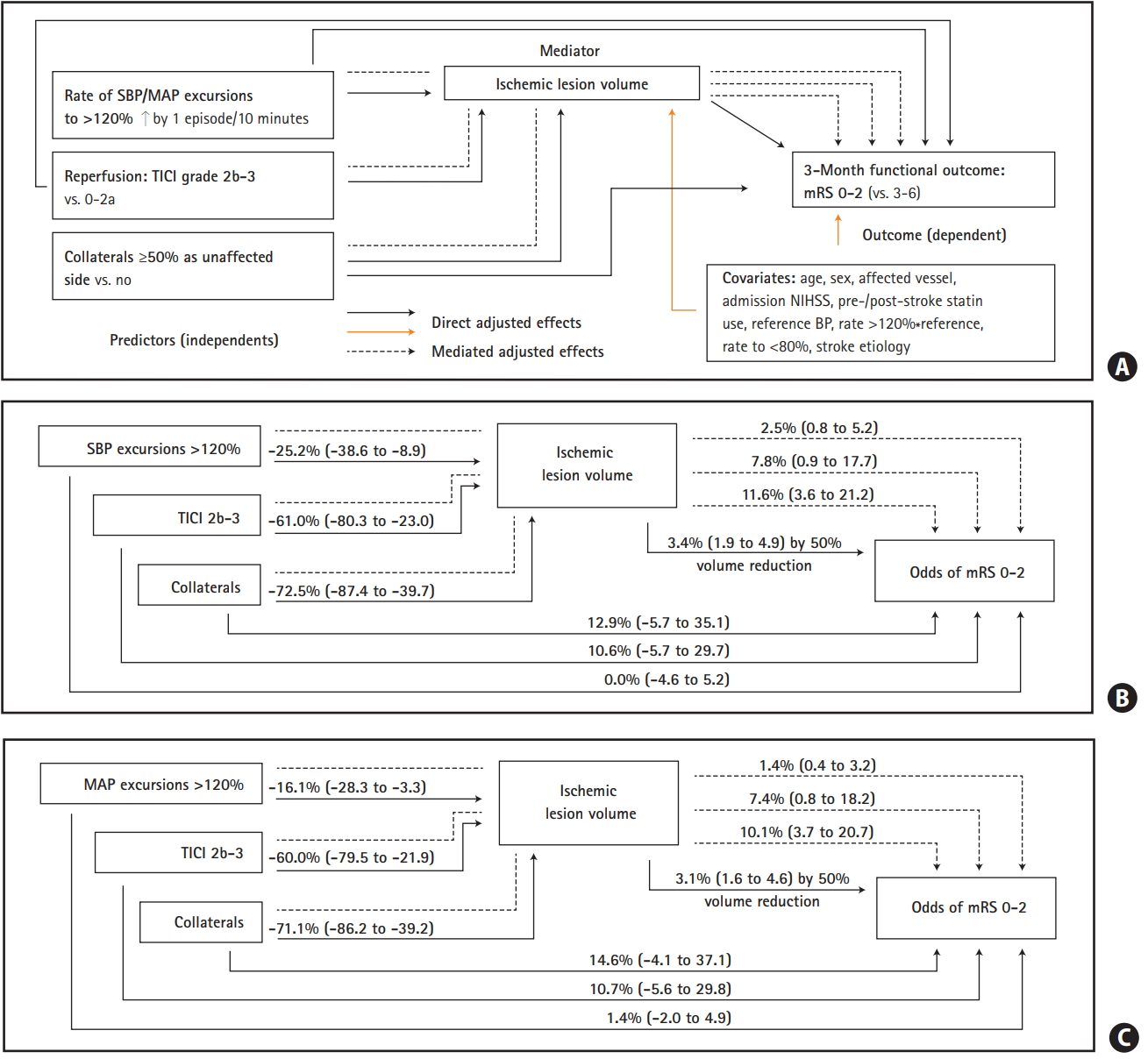
Full, reduced and final models were fitted to the outcome (see Supplementary Table 5 for complete models). Independent variables consistently not associated with mRS were consecutively removed (Figure 2). Final models are shown in Table 3. The rate of SBP/MAP excursions to <80% of the reference was not associated with the outcome (Table 3). When not accounting for ILV, higher rate of SBP/MAP excursions to >120%, TICI grade 2b-3, good collaterals and pre-index stroke statin use were associated with mRS 0-2 (Table 3, Model A). Higher onadmission NIHSS score, cardioembolic/unknown stroke etiology, post-index stroke statin use and older age were associated with lower odds of mRS 0-2 (Table 3, Model A). When accounted for, higher ILV was associated with lower odds of mRS 0-2 (Table 3, Model B). At the same time, the effects of SBP/MAP excursions, TICI grade and of collaterals were reduced to include unity (Table 3, Model B). Mediation analysis (Figure 4) showed an indirect (via ILV) association between higher rates of SBP/MAP excursions to >120% and mRS 0-2 (the same was shown for TICI 2b-3 and good collaterals).
Several models (Supplementary Table 5) indicated an interaction between the rate of SBP/MAP excursions to >120% and TICI grade: (1) a strong association between higher rates and mRS 0-2 in patients with TICI 2b-3 (n=115) and none in patients with TICI 0-2a (n=40) with point-estimates <1.0; (2) no association between TICI 2b-3 and mRS 0-2 in patients with zero excursion rates, with clear-cut associations between TICI 2b-3 and higher odds of mRS 0-2 at rates around 1.0/10 minutes and higher (Supplementary Table 5, Models final C, D). We consider final models without the interaction (Table 3) to more generally describe the data than the models with this (uncertain) interaction that did not indicate harms ascribable to SPB/MAP excursions (for the full rationale, see Supplementary Methods).
Discussion
We found that in anterior circulation stroke patients treated with EVT/rtPA, in whom BP was generally kept within the recommended limits, higher in-procedure SBP/MAP was associated with a better 3-month functional outcome. The findings are supported by the association of higher rates of in-procedure SBP/MAP excursions to >120% of the reference values, and of higher reference BP with mRS 0-2. The fact that no such association was observed for (higher) in-procedure mean BP is likely due to aliasing by the effects of a higher number of excursions over a high(er) reference value. A stronger association between BP excursions and in-procedure mean BP at higher reference BP supports such a view. Data also suggest associations between a higher rate of SBP/MAP excursions to >120% and lower ILV. Higher ILV was associated with lower odds of mRS 0-2, and mediation analysis that differentiates effects identifying indirect paths [21] plausible in a temporal and pathophysiological sense disclosed its mediator role: BP excursions are directly associated with lower ILV, lower ILV is directly associated with a better functional outcome, excursions affect functional outcome “through” the effects on ILV.
The analysis has limitations common to similar recent reports on the topic [13-16]—it did not account for the post-procedural BP; it did not test specific BP targets but evaluated spontaneously occurring patterns, where some, otherwise possible patterns, might not have occurred. Also, data on the initial infarct volume were not available. This leaves space for the assumption that patients with a larger initial infarct volume might have been managed at lower BP levels (to avoid hemorrhagic transformation), while a less stringent BP management might have been in place in patients with lower volumes, thus spuriously “grouping” poorer outcomes and lower BP (large initial volume), and better outcomes and higher BP (smaller initial volume). However, all observed associations were adjusted for on-admission NIHSS and use of antihypertensives between admission and EVT. It is reasonable to consider that these two variables to a large extent subsumed the “impact” of the initial infarct volume: if higher on-admission NIHSS (a “proxy” for larger infarct volume) would “go” together with higher on-admission BP, it would be associated also with immediate use of antihypertensives. However, our data showed that (1) higher on-admission BP but not NIHSS was associated with antihy-pertensive use; (2) BP reduction from admission to EVT (adjusted for on-admission BP) was similar in patients treated and not treated with antihypertensives; (3) neither on-admission NIHSS nor the use of antihypertensives were associated with reference BP or with in-procedure mean BP. Taken together, the findings suggest that the observed BP patterns were likely a consequence of the intended management within the recommended limits, and were not driven by the initial stroke severity (i.e., initial infarct volume). Furthermore, we consider invasive frequent BP recordings, inclusion of unselected patients, uniform anesthesia, and accounting for a number of confounders to be the study strengths.
Present findings apparently disagree with a similar recent report [13]. Individual in-procedure BP indicators (maximum, minimum, dips) were evaluated for association with 30-day mRS in 147 EVT-treated patients. In multivariate models (13 independents), higher maximum SBP was associated with lower odds of mRS 0-2. The only other significant effect was admission NIHSS, while collaterals, stroke etiology, ILV were not considered [13]. The cohort differed from ours in respect to anesthesia (46% GA), less common rtPA use (35.8%), fewer reperfusion successes (50%), lower mRS 0-2 achievement (17%), and fewer BP recordings (every 5 minutes) [13]. The apparently discordant results might be due to these methodological and cohort differences.
Three further similar studies indirectly support the present findings but also oppose them in a way [14-16]. All three studies suggest benefits of “higher” in-procedure BP, but imply this indirectly by recognizing detrimental consequences of low(er) MAP, i.e., in-procedure MAP dips, which we could not confirm. In one study (EVT under GA), at least one episode of MAP decline >40% from the baseline value was associated with 3-month mRS 3-6, but time spent at this MAP level was not [14]. Another (smaller) analysis (EVT under GA) reported no association between the largest in-procedure MAP decline from the baseline value and 3-month mRS. However, lower (vs. baseline) average in-procedure MAP was associated with poorer mRS, while higher average MAP was associated with better mRS [15], thus being in line with present results. Detrimental effect of low(er) in-procedure MAP was suggested also in EVT under conscious sedation—lowest in-procedure MAP <100 mm Hg was associated with 3-month mRS 3-6 [16].
Despite methodological differences between the present and previous reports, there is evidence of detrimental consequences of low in-procedure MAP [14-16]. This is in apparent disagreement with the reported association between high(er) SBP during the first 24 hours post-EVT and poor functional outcomes [9,22]. It seems that management of BP in anterior circulation acute stroke patients undergoing EVT requires different strategies: one focused on in-procedure targets and prevention of excessive dips, the other focused on the post-procedural period targeting lower levels with a prompt management of excessive peaks.