Introduction
Recanalization of the arterial occlusion is the cornerstone of treatment in acute ischemic stroke (AIS) patients. Several randomized clinical trials (RCTs) [1-7] and an individual patient data meta-analysis [8] have recently shown that mechanical thrombectomy (MT) combined with standard treatment (including intravenous thrombolysis [IVT]) was superior to standard treatment alone, with higher rates of reperfusion, more frequent favorable functional outcome, and lower 3 months mortality, for severe AIS caused by large-vessel occlusion (LVO) in the anterior circulation. The cumulative evidence from these studies resulted in the modification of practice guidelines and profound changes in worldwide stroke care organization [9].
Despite its compelling efficacy, up to half of AIS-LVO patients do not regain functional independence after MT [8]. This unfavorable outcome is largely attributable to unsuccessful mechanical recanalization [1-4,7]. Amongst factors influencing recanalization success, clot length is an important determinant [10-12], that was scarcely assessed in the recent RCTs. Indeed, if patients were included in case of LVO on computed tomography angiography (CTA), only few studies [13,14] assessed clot length using the CTA-defined clot burden score (CTA-CBS). These analyses demonstrated a direct link between clot length, likelihood of recanalization, final infarct volumes, and 3-month neurological outcome.
Brain magnetic resonance imaging (MRI), using the T2*-MRI sequence, is a powerful tool to identify thrombus in AIS patients, based on the presence of a susceptibility vessel sign (SVS) [15,16]. Clot length is included in the T2*-CBS [17], in which a lower score reflects longer thrombus. T2*-CBS was recently used after IVT or MT, as a predictor of recanalization and functional outcome [17,18]. However, as for CTA-CBS [19], these studies were mainly retrospective and no adjustment was performed for crucial baseline prognostic variables such as initial National Institutes of Health Stroke Scale (NIHSS) score or recanalization results.
With more than 300 patients included with pre-treatment MRI, the THRombectomie des Artères CErebrales (THRACE) trial (ClinicalTrials.gov, number NCT01062698) offers a unique opportunity to study the associations between T2*-CBS, successful recanalization rate and functional independence. The purpose of this prespecified post hoc analysis of the THRACE trial was to determine the relation between T2*-CBS and the effect on endovascular treatment and neurological improvement in AIS-LVO patients.
Methods
Study design
THRACE was a randomized controlled trial done in 26 centers in France. Study design and protocol have been previously detailed [7]. AIS-LVO patients were randomly assigned in a 1:1 ratio to receive either IVT alone (IVT group) or IVT+MT (IVTMT group). IVT had to be started within 4 hours and MT within 5 hours of symptom onset. Occlusions had to be confirmed by CTA or magnetic resonance angiography (MRA). Before randomization, written informed consent was obtained from all patients or their legal representatives. The study protocol was approved by the Comité de Protection des Personnes (CPP) III Nord Est Ethics Committee and the research boards of the participating centers. No data were reported on thrombus characteristics obtained on admission brain MRI.
Outcomes measures
The primary outcome in the THRACE trial was the proportion of patients with a score of 0-2 on the modified Rankin Scale (mRS), indicating functional independence, at 3 months after the intervention. Secondary outcomes nonexhaustively included, successful recanalization, defined as a modified Thrombolysis in Cerebral Infarction (mTICI) score ≥2b [20] in the IVTMT group, and the NIHSS score at 24 hours in all patients. Clinical assessments were done by vascular neurologists who were not masked to the treatment to which the patients had been allocated.
Image analysis
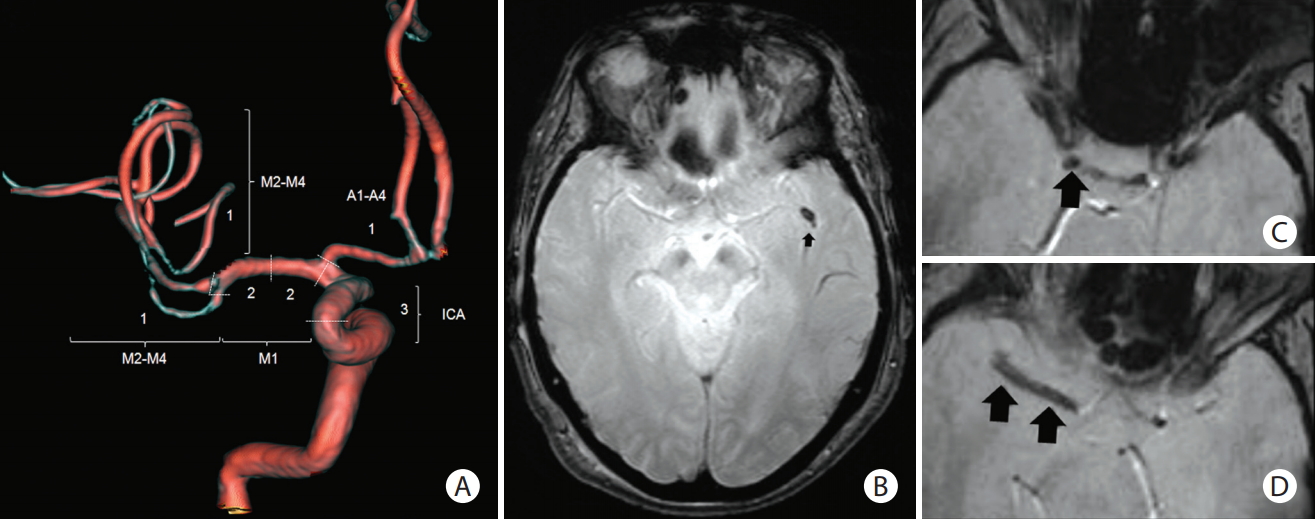
MRI images and angiograms before and after MT were reviewed by four experienced neuroradiologists, who were masked to randomization group and patient clinical outcome. Baseline examinations included the determination of the Alberta Stroke Program Early CT Score (ASPECTS) [21] on diffusion weighted imaging (DWI) sequence and the location of the arterial occlusion by MRA. After initial training, two experienced observers from the core imaging committee searched for SVS, that is, a hypointense signal on T2* within a vascular cistern, exceeding the size of the homologous contralateral arterial diameter. If present, an appropriate T2*-CBS was assigned according to the methods of Legrand et al. [17] T2*-CBS is a 10-point scoring system used to define the extent of thrombus in the anterior circulation (Figure 1). Because susceptibility artifact at the skull base prevents evaluation of the infraclinoid internal carotid artery (ICA), this segment was not analyzed and 3 points were assigned to the supraclinoid ICA level, for consistency with the CTA-CBS. A score of 10 implies clot absence. A score of 0 implies complete multisegment vessel occlusion by a long clot. T2*-CBS was subsequently dichotomized using a >6-point cut-off (0-6: long clot vs. 7-10: small clot), according to and for comparison with CTA-CBS studies [13].
Statistical analysis
All primary outcome analyses were performed according to the intention-to-treat principle. For this study, the primary effect variable was the proportional adjusted common odds ratio for a shift in the direction of better outcome on the 3-month mRS. The association between full-scale or dichotomized T2*-CBS (0-6 vs. 7-10) with shift in the direction of better outcome on the mRS was assessed using ordinal logistic regression respectively.
For all outcome parameters, two models were generated as previously used [13]. Model A contained the T2*-CBS variable and treatment. In model B, the main prognostic baseline variables were added: age, stroke severity (NIHSS score), glycemia, and ASPECTS score. An interaction term of treatment allocation with T2*-CBS was added to the both unadjusted and adjusted models to assess whether T2*-CBS was a treatment effect modifier. The models with and without added interaction term (nested models) were compared using the chi-square test.
Patient characteristics are reported for groups with and without SVS and patient with long (T2*-CBS 0-6) and small clot (T2*-CBS 7-10). Continuous variables were compared with Student t-test, a Mann-Whitney test, or Median test, as appropriate. Categorical variables were compared using chisquare or Fisher exact test, as appropriate.
For all statistical analyses, P<0.05 was considered statistically significant. All statistical analyses were done with SAS/STAT version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Patient characteristics
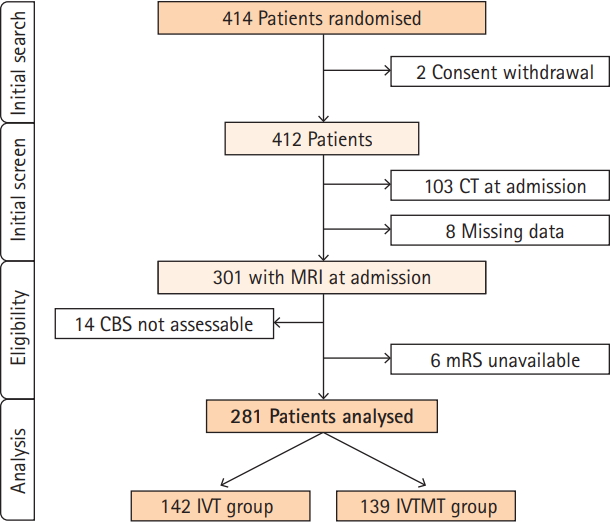
Among 414 patients randomized in the THRACE trial (Figure 2), initial imaging work-up was performed using MRI in 153 of 208 patients (74%) in the IVT group and 148 of 204 patients (73%) in the IVTMT group (P=0.83). Of these, 20 patients were excluded leaving 281 patients for analysis in the present study. Baseline characteristics are summarized in Supplementary Table 1. Sociodemographic characteristics, comorbidities, and baseline NIHSS did not differ between IVT and IVTMT groups, nor delays from symptom onset to IVT initiation or to randomization.
Baseline characteristics according to T2*-CBS group
Among 281 patients included in 19 centers, 234 (83.3%) demonstrated presence of SVS, 118 (50.4%) in the IVT group, and 116 (49.6%) in the IVTMT group. Overall, the median T2*-CBS was 7 (interquartile range, 6 to 8), similar in IVT and IVTMT groups (P=0.38). After dichotomizing the T2*-CBS, 111 patients (39.5%) had a long clot and 170 (60.5%) a small clot. Patients with a long clot were significantly older, had a lower DWI-ASPECTS score, more often had diabetes mellitus or were active smokers at baseline (Table 1).
Primary outcome
The primary outcome was assessed in 281 patients (Table 2). At 3 months, 79 of 139 patients (56.8%) in the IVTMT group and 65 of 142 (45.8%) in the IVT group had functional independence. The primary outcome was not influenced by the presence of a SVS (120/144 in mRS 0-2 and 114/137 in mRS >2, P=0.98).
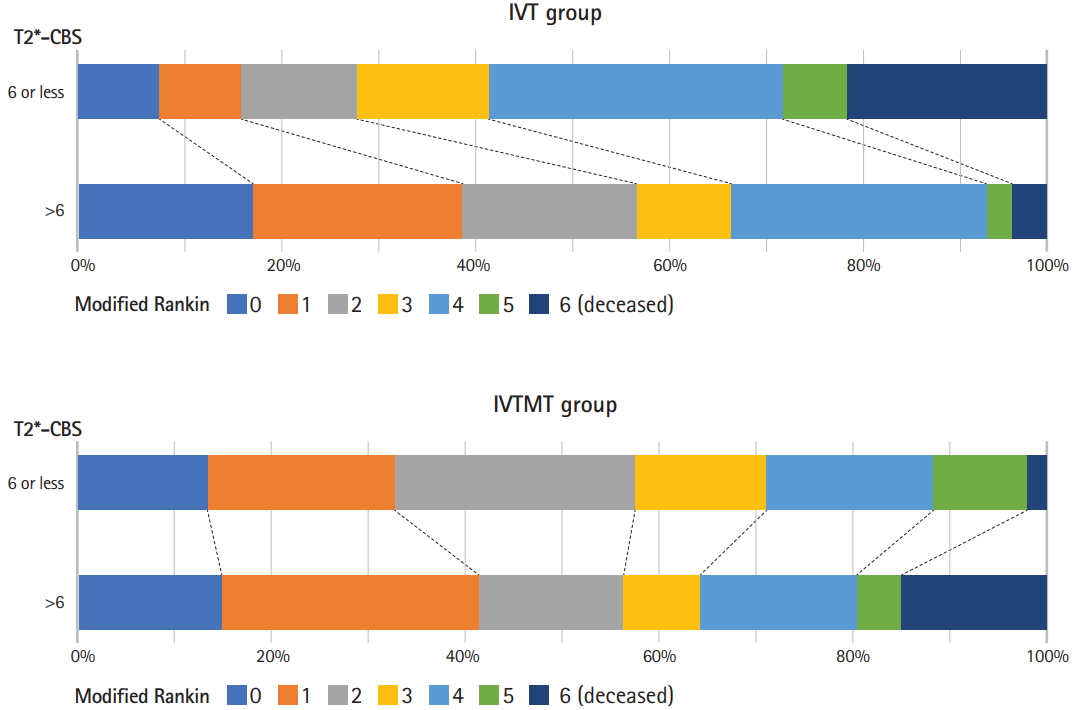
Proportion of small clot was significantly higher in patients with favorable (97/144 patients, 67.4%) than in patients with unfavorable outcome (73/137, 53.3%; OR, 1.81; 95% confidence interval [CI], 1.12 to 2.94; P=0.016). Small clot was associated with a shift toward better outcome on the mRS; proportional odds ratio (POR) per each T2*-CBS point was, with randomization group adjustment: 1.19 (95% CI, 1.05 to 1.34), 1.34 (95% CI, 1.13 to 1.59), and 1.04 (0.87 to 1.23) (interaction, P=0.03) in the whole population, in IVT and IVTMT groups, respectively. After adjustment, the effect of the full scale T2*-CBS was not statistically significant in the whole population (POR, 1.12; 95% CI, 0.99 to 1.27; P=0.1) and for the IVTMT group (POR, 0.94; 95% CI, 0.79 to 1.12; P=0.73) but remains significant for the IVT group (POR, 1.32; 95% CI, 1.11 to 1.58). Considering the dichotomized T2*-CBS, similar results were found (Table 3 and Figure 3).
Secondary outcomes
Successful recanalization was observed in 66 of 91 patients (72.5%) in the IVTMT group who received MT treatment. There was no association between the presence of SVS and recanalization result (P=0.45) nor influence of the T2*-CBS, considered as a continuous variable (P=0.75) or dichotomized (7-10 vs. ≤6, P=0.57) (Supplementary Table 2).
Discussion
In this prespecified post hoc analysis of THRACE trial, longer clot as assessed using T2*-CBS was associated with a higher likelihood of unfavorable neurological outcome. In analysis of 3-month ordinal mRS, adjusted on randomization group, there was a 19% relative increase in the likelihood of a worse outcome with every point decrease in T2*-CBS. Despite the worst outcome with long clot, the relative benefit of IVTMT over IVT seemed to increase with longer thrombus.
We found a significant interaction between treatment allocation and clot length as measured using T2*-CBS. In the recent RCTs [1-7], evaluation of intracranial thrombus burden was performed on CTA. In the ESCAPE trial, Puetz et al. [22] demonstrated an increase in benefit from MT for lower CTA-CBS, i.e., longer thrombus, when compared with higher CTA-CBS. Similarly, in a post hoc analysis of 108 patients included in the THERAPY trial [14], longer thrombi, as defined on CTA, were independently associated with worse clinical outcomes. Furthermore, in adjusted analyses of 90-day ordinal mRS, there was a 33% relative increase in the likelihood of a worse outcome with every 5-mm increase in thrombus length and the relative benefit of MT compared with IVT alone increased with thrombus length [14]. Our results stand in apparent contradiction with the post hoc analysis of the MR CLEAN trial, which did not establish thrombus length as a treatment effect modifier [13]. In this latter study, the underestimation of the increased benefit of MT over IVT in longer thrombi can be tentatively explained by the fact that CTA may overestimate the extent of thrombus involvement. Indeed, if the collateral circulation is weak or with short delays between contrast injection and imaging acquisition [23], an overestimation of clot length is possible. In addition, although CTA has been demonstrated to provide accurate thrombus length measurement [24], it is less sensitive than MR susceptibility weighted sequences [25]. However, there are no comparative studies of clot length imaged with both CT and MRI.
The greater beneficial effect in IVTMT group accounts for the paradoxical finding of increasing relative benefit of MT despite the overall worse outcome associated with longer thrombi. This finding illustrates the difference between prognostic and therapeutic imaging biomarkers; in AIS-LVO patients, long clot is simultaneously a negative prognostic biomarker and a positive therapeutic biomarker with regards to MT (i.e., clot length modifies the differential treatment effect of MT or IVT). The detrimental effect of low CBS on clinical outcome is most likely attributable to greater difficulty of recanalizing longer and/or multisegment thrombi [14,24]. Other explanation of the worst outcomes seen in lower T2*-CBS may be that longer clot were associated with lower baseline ASPECTS. In case of longer clot, there is a higher probability of occlusion of the lenticulostriate and insula perforators, for which collateral compensation is limited. In addition, an inverse correlation between pial collaterals strength and clot length has been demonstrated [14]. Weaker collaterals may contribute to both the extent of the thrombus and a reduction in cerebral blood flow to the ischemic penumbra, potentiating the extent and degree of injury, hence contributing to worse clinical outcomes. Taken together, worst outcome seen with long clot is likely the consequence of a synergistic effect of poor collateral strength, larger baseline infarct and longer thrombotic occlusion that is difficult to rapidly recanalize.
In line with THERAPY trial results [14], we did not demonstrate any influence of the T2*-CBS on recanalization result, in the IVTMT group. As a difference, in our study, patients were not included based on clot length whereas in THERAPY trial, only patients harboring thrombi >8 mm were included. A non-randomized study of mostly stent-retriever (SR) MT also demonstrated no relationship between thrombus length, as measured on SVS, and successful recanalization [26]. Our study reinforces the idea that, if longer thrombi are unlikely to recanalize in IVT patients, length did not impact efficacy of MT.
Recently, randomized comparison of first-line MT with ADAPT technique versus SR did not result in an increased successful revascularization rate [27]. However, in the ASTER trial, thrombus length was short with mean values of 13 and 11.5 mm, in ADAPT and SR groups, respectively. Furthermore, in a recent post hoc analysis of the ASTER trial, the first-line MT strategy (aspiration vs. stent) did not result in an increased successful reperfusion rate in AIS-LVO patients according to the admission CBS [28]. Identifying the best MT method to address LVOs with long clot, i.e., T2*-CBS (0-6), will most likely be a challenge, notably because of the expected limited added benefit of a device association choice versus another, resulting in anticipated power issues. Knowledge of other thrombus characteristics, such as complex composition, tensile, compressive, rheological, and frictional properties, which might contribute to their relative resistance to clot removal during MT, may help in optimizing endovascular devices and strategies [29,30]. Until more data are available, clot length, assessed using T2*-CBS, is a reasonable approach to guide treatment strategies and select patients in future trials.
The strength of our study is that, beyond the demonstration of a LVO, no other imaging criteria was used to select patients in the THRACE trial. Hence, patients with unfavorable clinical and imaging profiles were included, resulting in generalizable findings. The present study was based on the largest to date AIS-LVO population initially included based on brain MRI data in a RCT and allows for a less biased assessment of the efficacy of baseline imaging prognostic biomarkers to select patients for future studies.
A few points may require clarification. First, 59 patients randomized to the intervention arm did not receive MT. When evaluating imaging biomarker of efficacy for MT, it could add to the sensitivity of the analysis to only include the patients who actually received MT. A second limitation is that T2*-CBS likely underestimates full clot extent, given that the susceptibility effect depends on thrombus composition and age [15]. An additional limitation is the variability in MRI measurement [31]. Indeed, the extent of the SVS blooming artifact might vary with different magnetic field strengths and echo time. Future studies should examine the impact of imaging acquisition parameters on the T2*-CBS variability. Finally, 47 of 281 patients did not demonstrate SVS and were included in the analysis as T2*-CBS=10. This may have underestimated the real clot length in these patients.
Conclusions
Clot length, as assessed using the MRI based T2*-CBS is independently associated with functional outcome in patients with AIS caused by a LVO, and may be used as prognostic biomarker. Despite the worst outcome with long clot, the relative benefit of MT over IVT seemed to increase with low T2*-CBS.