Tobacco Use: A Major Risk Factor of Intracerebral Hemorrhage
Article information

Abstract
Spontaneous intracerebral hemorrhage (sICH) is one of the deadliest subtypes of stroke, and no treatment is currently available. One of the major risk factors is tobacco use. In this article, we review literature on how tobacco use affects the risk of sICH and also summarize the known effects of tobacco use on outcomes following sICH. Several studies demonstrate that the risk of sICH is higher in current cigarette smokers compared to non-smokers. The literature also establishes that cigarette smoking not only increases the risk of sICH but also increases hematoma growth, results in worse outcomes, and increases the risk of death from sICH. This review also discusses potential mechanisms activated by tobacco use which result in an increase in risk and severity of sICH. Exploring the underlying mechanisms may help alleviate the risk of sICH in tobacco users as well as may help better manage tobacco user sICH patients.
Introduction
Hemorrhagic stroke occurs following blood vessel rupture-induced bleeding into the brain [1]. In parenchymal hemorrhage, a hematoma forms with or without extension into the ventricles [2]. Spontaneous intracerebral hemorrhage (sICH) accounts for about 10% of all strokes [1,3]. The incidence rate varies by geographical location. The sICH percentage of total strokes is higher in Japan and Korea than in the USA, UK, and Australia [1,4]. A systematic review of population-based studies and comparison of incidence rates of sICH in high income and low to middle income countries observed that the rates of primary sICH in low to middle income countries are almost double of that in high income countries [5]. The incidence rate in the developed world has remained stable over the last three decades [4,6]. A population-based study that compared changes in incidence and etiology of sICH in Oxfordshire, UK between 1981 and 2006 observed that the incidence of sICH is decreasing in the population aged <75 years while increasing in the population aged >75 years without any overall change in the incidence rate [7].
sICH results from the rupture of parenchymal blood vessels mainly within the basal ganglia, thalamus, pons, or cerebellum [8]. Characteristic symptoms for sICH diagnosis include rapidly progressive neurological signs and symptoms, headache, vomiting, seizures, and reduced consciousness [9]. sICH is the deadliest stroke sub-type with a 30-day mortality of over 40% [10-12]. The 1-month mortality rate varies depending on the location of the hemorrhage [8]. Less than half of sICH patients survive 1 year post-ictus, and about one-third survive for 5 years [13]. The median case fatality is lower in Japan (16.7%) compared to the rest of the world (42.3%) [11]. Only 21% of sICH patients are able to lead an independent life at 6 months [14]. Currently, there is no proven therapy to prevent hematoma expansion in sICH patients, and thus clinicians are unable to offer more than supportive care.
Hematoma expansion
Hematoma growth early after ictus is common in sICH patients [10]. The majority of hematoma expansion occurs during the first 4 hours post-symptom onset; however, hematoma expansion with a wide degree of variability continues in patients during the first day [10,15]. This is mainly due to variable duration between baseline and a follow-up scan as well as in the threshold used for expansion. Hematoma expansion is defined as an increase of hematoma volume on a repeat computed tomography (CT) by 33% to 50% (or an absolute change in hematoma volume of 12.5 to 20 mL) [16]. An earlier review article noted that about 73% of patients experience some expansion in hematoma volume and about 33% of them experience a larger than 33% growth in hematoma volume [8].
Early hematoma growth is also associated with neurological deterioration when evaluated using Glasgow Coma Scale and National Institutes of Health Stroke Scale scores [10]. The hemorrhage volume is considered a powerful predictor of 1-month mortality and morbidity in sICH patients [17]. An earlier study reported that for deep hemorrhages, a smaller hematoma volume (<30 mL) resulted in a lower 1-month mortality (23%), while a larger hematoma volume (>60 mL) resulted in a higher 1-month mortality (93%) [17]. Davis et al. [18] performed a meta-analysis of three prior clinical studies to determine if subsequent hematoma growth further increases the risk of poor outcomes in sICH patients. They observed that each mL increase in hematoma volume resulted in a 1% increase in the risk of death. They also observed that every 10% increase in hematoma growth resulted in a 5% increase in the risk of death, and that hematoma growth is also an independent determinant of poor functional outcome [18]. These clinical studies indicate that preventing hematoma growth in sICH patients may result in improved outcomes in these patients.
Mechanisms of injury
An artery rupture results in initial bleeding. This initial bleeding and related hypertension results in hematoma expansion leading to physical damage to the surrounding cells and cellular architecture. This phenomenon is described as “mass effect.” [19] Larger hematoma expansion results in a midline shift, causing physical damage in areas remote from the bleeding site. Hematoma and surrounding edema lead to an increase in intracranial pressure (ICP). This increase in ICP may also cause a decrease in cerebral perfusion pressure causing ischemia/oligemia injury to the brain [20]. These are primary mechanisms of injury following sICH.
Pathways activated by the primary injury and hematoma cause secondary brain injury following sICH. Once the hematoma is stable, thrombin levels increase as a part of hemostasis. This increase in thrombin levels activates several cell-damaging pathways including infiltration of inflammatory cells, proliferation of mesenchymal cells, scar formation, brain edema, seizures, microglial activation, and both astrocytic proliferation and death [19,21,22]. There is also a breakdown of the blood-brain barrier (BBB), which also contributes to secondary brain injury [23]. BBB breakdown is believed to support activation of the complement system and subsequent erythrocyte lysis [19]. The iron from hemoglobin and carbonic anhydrase 1 released during hematoma resolution also contribute to secondary brain injury [19]. BBB breakdown and blood components can also activate microglia [21,24]. Microglial activation is one of the major sources of secondary brain damage after sICH, as microglia release various inflammatory mediators and activate astrocytes to release proinflammatory cytokines [21,24,25]. In a rat model of intracerebral hemorrhage (ICH), microglial activation was seen within 1 hour after collagenase-induced ICH and remained at increased levels up to 3 to 4 weeks afterwards [24]. Furthermore, other cell death mechanisms such as excitotoxicity, seizures, spreading depression, and activation of cell death pathways also play a role in secondary brain injury [19].
Etiology
Risk factors for sICH include comorbidities such as hypertension, cerebral amyloid angiopathy, and chronic liver disease. Medication-associated risk factors for sICH are antiplatelet therapy, anticoagulant treatment, and selective serotonin reuptake inhibitors [1,4,6,9]. Non-modifiable risk factors for sICH include older age and male sex. Modifiable risk factors include alcohol consumption, cigarette smoking, and cholesterol/diet [1,4,6,9]. An earlier study observed that older (≥55 years of age) sICH patients with low and high body mass index (BMI) are associated with deep sICH when compared with those with normal BMI [26]. The same study did not find any effect of BMI on lobar sICH [26]. Although the relative risk (RR) of sICH is higher in men compared to women, the severity of sICH is greater in women compared to men [6,27,28]. The risk ratio for sICH is also higher in blacks and Hispanics [27]. Apolipoprotein E 2 and 4 alleles are also risk factors for sICH [6]. Besides, Genome Wide Association Studies identified several genetic loci that are associated with the risk of sICH [29]. Hypercholesterolemia and a high intake of fruits and vegetables are associated with a reduced risk of sICH [6].
Although the overall incidence rate of sICH has not changed over the past 30 years, the risk factor profile has changed [6]. An earlier study identified that the incidence of hypertension-associated sICH decreased over time; however, the incidence of sICH associated with the use of antithrombotic medication increased over the same time period [7]. With an increase in the incidence of antithrombotic use-associated sICH in older individuals and an expected increase in the prevalence of amyloid angiopathy with a growing aging population, the overall number of cases of sICH is expected to increase in the future [7].
Relationship between tobacco use and ICH
One risk factor of major concern is cigarette smoking as seen in Figure 1. Tobacco use is one of the leading causes of preventable death in the world [3]. Although the smoking rate has decreased (from 41.2% in 1980 to 31.1% in 2012), owing to population growth, there has been an increase in the number of current cigarette smokers in the world (from 721 million in 1980 to 967 million in 2012) [30]. Nicotine, the major toxic agent in the complex chemical mixture of cigarette smoke which contains more than 9,000 different chemicals, increases the risk of cardio-/cerebrovascular disease [31]. As mentioned, tobacco use is well-recognized as one of the major risk factors for sICH [32-40]. Table 1 summarizes the results of several original studies evaluating the risk of sICH in current tobacco users worldwide [33,37,41-52]. Only studies that included greater than 40 sICH cases and that specified confirmation of ICH with either cranial CT imaging, CT angiography, or magnetic resonance imaging were included in the list [53]. These studies clearly indicate that tobacco use increases the risk of sICH across various ethnicities and populations, although this risk is not uniform. Tobacco use is one of the most frequent risk factors for sICH in young people, and smoking is most prevalent in young sICH patients [54-56]. This is of particular concern as greater than 30% of men and 20% of women between ages 20 to 49 years smoke daily [30]. The risk of sICH recurrence in survivors of sICH is about 1% to 3% per year [57]. An earlier study evaluating factors for recurrence of sICH identified tobacco use as one of the risk factors [58].
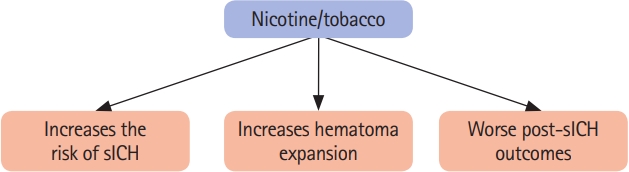
A schematic diagram summarizing the impact of nicotine/tobacco use on the risk of spontaneous intracerebral hemorrhage (sICH) and outcomes following sICH.

Risk of ICH in current tobacco users
Several studies also looked at the difference between the risk of sICH in currently smoking men and women (Table 2) [34,43,48,59,60]. Two clinical studies found that incidence of sICH is higher in males compared to females [61,62]. Another study reported that males have a higher risk for hematoma expansion (odds ratio [OR] of 1.7) following sICH than females [63]. The Japan Public Health Center-based Prospective Study on Cancer and Cardiovascular Disease (JPHC) Study followed smokers without a history of stroke, coronary heart disease, or cancer from the early 90s to the end of 2001 and observed that the RR of parenchymal hemorrhage was higher in smoking women compared to smoking men [59]. Another study that performed a pooled analysis of three large-scale cohort studies in Japan reported that the hazard ratio (HR) for sICH was 1.27 and 1.87 in male and female current smokers, respectively [60]. On the contrary, a study by the Midland (England) Cerebrovascular Research Group observed that compared to non-smokers, the adjusted RR for sICH was 1.82 and 1.3 in male and female smokers, respectively [34]. It is important to note that tobacco use affects the hormones estrogen and testosterone. An earlier study found that estrogen has a protective effect on intracranial aneurysm rupture, which is commonly associated with subarachnoid hemorrhage (SAH) [64]. Because cigarette smoking has anti-estrogenic effects, it is plausible that cigarette smoking may cause an increased risk of sICH in women by removing this protection [65]. The effect of tobacco use on testosterone levels in men are inconclusive [65]. Several studies reported that tobacco use increases testosterone levels in men, and one study found that increased testosterone may worsen behavioral outcome in a rodent model of sICH [66-69]. However, further confirmatory studies in a large population are needed to reach a definite conclusion in this regard. Although a general increase in the risk of sICH is seen in all current tobacco users, whether tobacco use has a sex-specific effect with respect to increasing the risk for sICH is inconclusive so far.

Relationship between sex and risk of sICH in smokers
To assess if there is a potential dose-response relationship between tobacco consumption and the risk of sICH, several studies evaluated the risk of sICH based on the number of cigarettes smoked. As can be seen from Table 3, an increasing number of cigarettes consumed daily mostly correlate with an increased risk of sICH [35,36,59,70-73]. In some of the studies, it appears that the risk of sICH decreases with increasing number of cigarettes consumed daily [41,59,74]. One potential explanation is ethnic differences. In Table 3, the first three studies were conducted in Caucasian majority countries, while the latter four studies were conducted in Asian countries. Differences in the rate of passive smoking in Asian and Caucasian majority countries may also provide an additional explanation for these differences. It is plausible that a higher rate of passive smoking in Asian countries may lead to increased baseline risk of sICH, and this may result in a potential ceiling effect, which may prevent a further dose-dependent increase in the risk of sICH in smokers. This conjecture is also supported by an earlier meta-analysis by Price et al. [42]. They observed that the risk of sICH in current cigarette smokers was higher in European and North American studies when compared to Asian studies. Also, because cigarette smoking is a risk factor for several other conditions, it is plausible that this decreased incidence rate in greater tobacco consumption group may be due to death from other conditions [75]. However, this remains to be investigated via an appropriate clinical study. Overall, clinical studies identify tobacco use as one of the major risk factors for sICH. Studies also establish a dose-response relationship between tobacco consumption (i.e., cigarette smoking) and the risk of sICH. Despite several clinical studies indicating the deleterious effects of smoking/tobacco use in sICH patients, there are no confirmatory systematic preclinical studies evaluating the effects of smoking on the risk of sICH. Future studies investigating the effect of tobacco use on the risk of sICH with adequate power are needed in the field.

Relationship between smoking frequency and risk of sICH
Smokers are known to have other comorbidities which may further predispose them to an increased risk of sICH. For example, tobacco use is shown to further increase the risk of sICH when in combination with other genetic risk factors and conditions such as hypertension, alcohol use, and pregnancy [76-78]. Tian et al. [78] observed an increased risk of sICH in hypertensive sICH patients with COL1A2 rs42524 polymorphism, especially when accompanied by alcohol consumption and tobacco use. One study found that cigarette smoking more than doubles the risk of sICH in hypertensive persons [79]. Another study found a 19% increase in the risk of sICH with a 10 mm Hg increase in systolic blood pressure level in smokers than in never smokers [77]. A Finnish study observed a U-shaped dose-response relationship between alcohol consumption in male smokers and sICH risk, with a 82% increased risk of sICH in heavy drinkers (>5 drinks per day) when compared to non-drinkers [80]. One British study also found that aspirin use on the previous night combined with current smoking increased the risk of sICH by 40% [81]. Furthermore, cigarette smoking is an important risk factor for developing type 2 diabetes [82], and several studies demonstrated that diabetes is also another risk factor for sICH [42,83-85]. Smoking may have a synergistic effect on diabetes patients, which may further increase the risk of sICH. These studies highlight that tobacco use itself directly and indirectly increases the risk of sICH.
Outcomes following sICH in tobacco users
Besides increasing the risk of sICH, earlier clinical studies also established that tobacco use also worsens outcomes following sICH (Figure 1). Smoking is considered as an important predictor of substantial hematoma expansion (SHE), short- and long-term mortality, and poor outcome in sICH patients [86-88]. As mentioned previously, hematoma expansion occurs in the majority of sICH patients following ictus. The risk of post-ictus hematoma expansion is higher in tobacco-using sICH patients. An earlier study that evaluated SHE (an absolute increase in ICH volume >6 mL or an increase >33% on the follow-up CT) in sICH patients demonstrated that the risk of SHE between 12 and 72 hours is significantly higher (OR, 2.527; P=0.023) in currently smoking sICH patients than in non-smoking sICH patients [88]. For this reason, the study included current smoking as one parameter to calculate the Hematoma Expansion Prediction Score [88]. A linear regression analysis found a significant correlation between daily cigarette smoking consumption and intracerebral hemorrhagic volumes in sICH patients [89].
As cigarette smoking increases the risk of hematoma expansion, it also increases the risk of poorer outcomes and death from sICH (Figure 1). Based on the Johns Hopkins clinical stroke database and the Nationwide Inpatient Sample database, Faigle et al. [86] observed that black (OR, 3.31; P=0.074) and white (OR, 7.42; P=0.010) smoker sICH patients had a higher risk of in-hospital mortality. Another study by Saloheimo et al. [87] evaluated risk factors for death in sICH patients (n=140) that survived the acute phase (3 months) and compared their long-term prognosis with the control population (n=206). They observed that during their 7-year follow-up, RR of death was significantly (P=0.043) higher in smoker sICH patients (RR, 3.09) than in the control population (RR, 2.73) [87]. Furthermore, one prospective study found that cigarette smoking was associated with an increased risk of death from sICH (RR, 1.9) [90]. This accumulation of evidence suggests that tobacco use increases hematoma volume and is linked to worse outcomes in sICH patients (Figure 1).
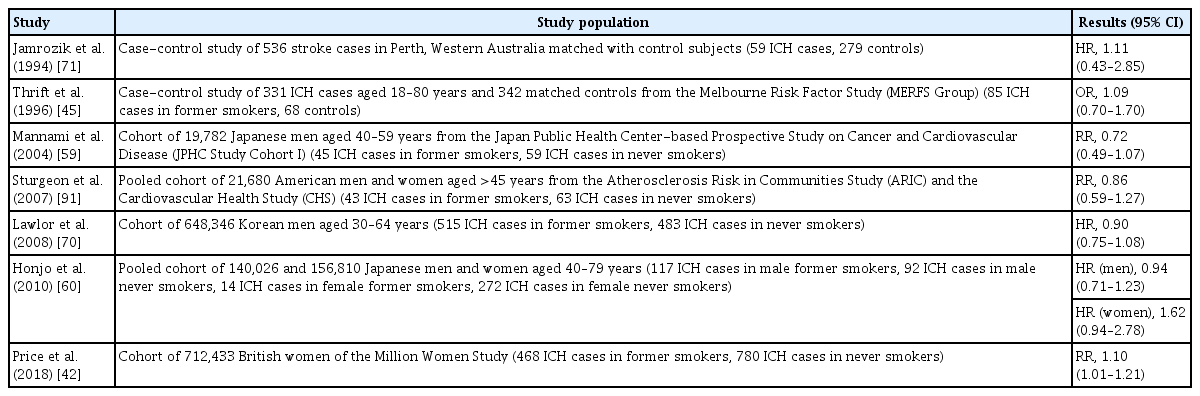
Former tobacco users and sICH
Most of the clinical studies merged former smokers into one non-smoker category, so limited studies are available that investigated the risk of sICH in former smokers. Some of these studies are summarized in Table 4 [42,45,59,60,70,71,91]. A cohort study in Korean men identified that quitters (HR, 0.75) and sustained (smoking status consistent from beginning to end of study period) ex-smokers (HR, 0.70) had a lower multivariable-adjusted risk of hemorrhagic stroke compared to non-reducing heavy smokers [92]. A British study similarly observed that ex-smokers were able to reduce their risk of sICH by at least 38% compared to current smokers. This risk reduction was even seen in former smokers that had quit less than 2 years prior to the study [43]. One Swedish study of women aged 30 to 50 years found an increased age-adjusted risk of sICH in former smokers (RR, 1.6) compared to non-smokers, although this study had a limited number of subjects [44]. Furthermore, a 10-year multicenter prospective study from China observed that the risk of hemorrhagic stroke remains higher in former male smokers (HR, 1.77). However, this study also reported that the risk of hemorrhagic stroke is lower in former female smokers (HR, 0.84). Owing to limited cases of SAH and to improve the statistical power, this study combined sICH and SAH cases in a single hemorrhagic stroke group [93]. A British study found a slight but significant increase in the risk of sICH of former smokers [42]. On the other hand, several studies found no difference between former smokers and never smokers, indicating that risk reduction in former smokers returns to that of never smokers [42,45,70,71,91]. However, owing to their limited number of former smokers, many of these studies do not differentiate former smokers based on how long they previously smoked, how much they previously smoked, and how long it has been since they quit smoking. Furthermore, the studies in Table 4 either did not specify how former smokers were defined, or those that did had varying definitions. Overall, these studies are inconclusive and a more detailed study in a larger population may help evaluate the risk of sICH in former smokers.
Relationship between former smoking and risk of sICH
Secondhand smoking/passive smoking and sICH
Although the field lacks extensive studies investigating the effects of secondhand smoking on sICH, its effects are similar to the effects of chronic active smoking, and there is a significant morbidity and mortality associated with secondhand smoking [94,95]. This is of particular concern as over a third of the world population is exposed to passive smoking [95]. Furthermore, nicotine has been found in the urine of non-smokers that share an immediate environment with smokers [96]. Nicotine in non-smokers, owing to the potential effect of passive smoking, may be responsible for undercalculating sICH risk and dampening the benefits of smoking cessation [60]. This is especially important in countries such as China, Japan, and South Korea, where there is a significant gap in smoking rates between men and women and where secondhand smoking may have a bigger impact [30,59,97,98].
Several studies found an increased risk of death from hemorrhagic stroke in passive smokers [99-101]. A Japanese study found a significant increased risk (35%) of death from sICH in never-smoking women exposed to secondhand smoking than never-smoking women without secondhand smoking exposure [100]. This risk increased to 64% when the women (aged 40 to 79 years) lived with a smoking spouse and another smoking family member. One Chinese study observed a significantly increased risk (22%) of death from sICH in passive smokers and an increasing risk of death from hemorrhagic stroke with an increasing quantity of cigarettes smoked by spouses [101]. In contrast, other studies did not find any association between passive smoking and hemorrhagic stroke [102,103]. However, these studies had a limited number of participants, combined sICH cases and SAH cases together as hemorrhagic stroke cases, and/or differed in how they measured secondhand smoking (i.e., exposure from home vs. workplace, exposure from spouse vs. family member, number of years exposed, and number of cigarettes smoked by spouse). Furthermore, none of these studies measured the nicotine content in the passive smokers’ systems. In general, these studies are inconclusive, and a more detailed, larger study is needed to identify any risk of sICH in passive smokers.
Potential mechanisms by which tobacco use affects the risk of sICH and outcome following sICH
Earlier clinical/epidemiological studies convincingly established that: (1) tobacco use/smoking substantially increases the risk of sICH [32-40], (2) smoker sICH patients have a higher risk of in-hospital mortality and poor outcome [86,87], (3) current smokers have an increased risk of hematoma expansion [88], and (4) there is a correlation between daily cigarette smoking consumption and intracerebral hemorrhagic volumes in sICH [89]. However, the underlying mechanisms are not well understood.
Tobacco use is known to activate multiple mechanisms that may contribute to an increased risk of sICH as well as worse outcomes following sICH. Figure 2 highlights some possible mechanisms by which tobacco or nicotine use may increase the risk of and worsen outcomes following sICH. Although chronic tobacco use is not associated with increased blood pressure, it is well established that nicotine transiently increases blood pressure when a person is smoking [31]. Activation of the sympathetic nervous system leads to the activation of nicotinic acetylcholine receptors, which in turn leads to an increase in heart rate and also blood pressure [31]. Increased risk of hypertensive heart disease, renal failure, and intestinal ischemia in smokers indicate poor vascular function [104]. It is plausible that this transient increase in blood pressure and impaired vascular function in tobacco users may increase the risk of sICH (Figure 2).
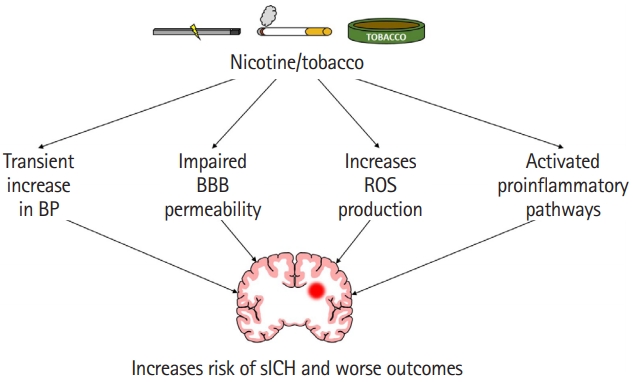
A cartoon highlighting various pathways responsible for increased risk of spontaneous intracerebral hemorrhage (sICH) and worse outcomes following sICH in nicotine/tobacco users. BP, blood pressure; BBB, blood-brain barrier; ROS, reactive oxygen species.
However, one contradiction is that cigarette smoking is well known to activate platelets, increase procoagulant activity, elevate fibrinogen levels, and cause plaque formation and rupture [105-108]. In that case, theoretically, this should result in decreased hematoma expansion and a better prognosis for the smoker. One Japanese group found some improvement in animal models, although nicotine treatment was given after sICH induction and no improvement was seen in hematoma volume [109,110]. A small Korean study found that cigarette smokers had better functional outcomes than non-smokers [111]. However, cigarette smoking and nicotine had a detrimental effect in sICH patients in clinical studies (Table 1) and in animal models from our laboratory (data not published). Some clinical studies also confirmed that no beneficial effect was seen after 3 months in sICH smoking patients [112,113]. The procoagulant benefit of cigarette smoking does not seem to be enough to overcome its detrimental effects.
In contrast, exposure to cigarette smoke causes denser fibrin clots and impairs fibrinolysis [107]. One study found depleted tissue plasminogen activator (tPA), a protease responsible for fibrinolysis and thrombolysis, in the brain capillaries of nicotine-treated rats compared to the control group [114]. Other studies showed increased levels and activity of plasminogen activator inhibitor-1, an inhibitor of tPA [107]. This could possibly lead to slower hematoma resolution, resulting in more damage and worse long-term outcomes in smoking sICH patients.
Cigarette smoking also weakens vessel wall integrity (Figure 2). Several studies found increased circulating endothelial cells and/or anuclear carcasses in the blood of humans right after smoking or inhaling cigarette smoke [115,116]. Another study found an increase in anuclear endothelial cells in the blood of rats following nicotine (equivalent to smoking of one cigarette) administration [117]. A study found increased OR of cerebral microbleeds in current smokers compared to non-smokers [118]. Cerebral microbleeds increase the risk of sICH, especially in Asian populations and in recurring ICH patients [119,120], which may explain the increased risk of sICH in the Asian population [1,6]. Another possible pathway could be through the effect of tobacco use on the risk of intracranial aneurysms. Some studies found that cigarette smoking and female sex increases the risk of multiple and larger aneurysms [121,122]. Arterial vessel damage and an acute increase in blood pressure could lead to an increased risk of rupture and intracerebral hemorrhage [123].
One of the potential mechanisms by which tobacco use increases hematoma expansion is by increasing BBB permeability (Figure 2). An earlier study observed that chronic treatment with smokeless tobacco products increases circulating levels of proinflammatory cytokine tumor necrosis factor α (TNF–α) [124]. Furthermore, chronic exposure of young mice to nicotine for 2 weeks resulted in increased expression of proinflammatory cytokines, chemokines, and adhesion molecules in brain microvessels [125]. This study reported that the levels of TNF–α increased by 12- and 14-fold in brain microvessels and brain tissue of animals exposed to chronic nicotine treatment than in control animals. Increased levels of TNF–α impairs barrier properties of the endothelium by affecting multiple pathways [126]. One of the pathways by which TNF–α impairs BBB properties is by affecting the dispersion of platelet-endothelial cell adhesion molecule-1 (PECAM-1) potentially via increasing PECAM-1 phosphorylation [127,128]. An earlier review article identified TNF–α stimulation-induced altered PECAM-1 dispersion as one of the major pathways by which TNF–α increases barrier permeability [126]. Overall, the literature indicates that chronic nicotine exposure weakens the integrity of BBB via increased levels of TNF–α (Figure 2).
Furthermore, chronic nicotine treatment is also shown to impair BBB function as evident by increased sucrose permeability, lower expression of the tight junction protein zona occludens 1 (ZO-1), and lower reactivity of claudin-3 in endothelial cells [129,130]. Increased BBB permeability is associated with an increased risk of bleeding in the brain. For example, early increase in parenchymal gadolinium enhancement, an indicator of compromised BBB, after thrombolytic therapy to ischemic stroke patients is significantly associated with an increased risk of hemorrhagic transformation [131]. This weakened BBB integrity may lead to a larger hematoma following rupture of cerebral vessels. Given that a small increase in hematoma volume significantly increases mortality in sICH patients, it is plausible that observed higher mortality and poorer outcomes in smoker ICH patients may be due to increased hematoma expansion/volume in this patient population [17].
Although nicotine is the most frequently studied component of cigarette smoking, cigarette smoke exposure also compromises BBB integrity (Figure 2). This is of particular concern as cigarette smoke affects not only firsthand smokers but also secondhand smokers. One study found that when brain microvascular endothelial cells (HBMEC: a model of human BBB) are exposed to tobacco smoke, cell viability decreased in a dose-specific manner and there was an increase in proinflammatory adhesion molecules [132]. This proinflammatory state could cause disruption of the BBB [133]. Furthermore, tobacco smoke contains high amounts of nitric oxide, which could result in increased BBB permeability [133-135].
Another harmful effect of tobacco smoke is its effect on secondary brain injury, especially in terms of microglial and astrocytic activation and oxidative injury (Figure 2). One study found that treatment with nicotine-derived nitrosamine ketone, a major component of tobacco smoke, caused microglia and astrocyte activation in mouse brain [136]. Increased levels before sICH could result in a greater proinflammatory state after sICH in cigarette smokers compared to non-smokers. Earlier studies also established the role of cigarette smoke exposure on reactive oxygen species (ROS) production. Several studies demonstrated that the exposure of HBMEC to tobacco products leads to an increased release of ROS and reactive nitrogen species (RNS) [132,137]. Naik et al. [137] also established that tobacco smoke exposure leads to the release of proinflammatory cytokines (TNF–α and interleukin 6). Acute smoking is shown to reversibly inhibit mitochondrial complex IV activity in human peripheral blood mononuclear cells [138]. This increase in oxidative stress and increased release of proinflammatory cytokines in the brain have also been seen in animal models treated with nicotine-derived nitrosamine ketone [136,139]. Increased ROS/RNS release and increased activation of proinflammatory pathways and mitochondrial dysfunction are known to play a role in brain damage following hemorrhagic stroke [140-146]. Others also established the role of free radicals in sICH-induced brain damage [147-149]. Because nicotine exposure increases the activation of pathways involved in post-sICH brain damage, it is plausible that elevated activation of those pathways is enhanced postsICH, which in turn leads to increased brain damage.
Conclusions
Several clinical studies identify tobacco use as a risk factor for sICH both in women and men. There is a dose-response relationship between tobacco use and the risk of sICH. Tobacco use also worsens outcomes following sICH. Tobacco use activates several mechanisms that increases the risk of sICH as well as increases post-sICH damage. Further studies are required to conclusively evaluate whether quitting tobacco use reverses the increased risk of sICH and passive smoking increases the risk of sICH.
Notes
Disclosure
The authors have no financial conflicts of interest.
Acknowledgements
This work was sponsored by the James and Esther King Biomedical Research Grant (9JK08). Authors are grateful to Dr. Brant Watson for critical reading of this manuscript.