Golden Hour Thrombolysis in Acute Ischemic Stroke: The Changing Pattern in South Korea
Article information
 , Ji Sung Leeb, Beom Joon Kimc, Jong-Moo Parkd, Kyusik Kangd, Soo Joo Leee, Jae Guk Kime, Jae-Kwan Chaf, Dae-Hyun Kimf, Tai Hwan Parkg, Sang-Soon Parkg, Kyung Bok Leeh, Jun Leei, Keun-Sik Hongj, Yong-Jin Choj, Hong-Kyun Parkj, Byung-Chul Leek, Kyung-Ho Yuk, Mi Sun Ohk, Dong-Eog Kiml, Wi-Sun Ryul, Jay Chol Choim, Jee-Hyun Kwonn, Wook-Joo Kimn, Dong-Ick Shino, Sung Il Sohnp, Jeong-Ho Hongp, Man-Seok Parka, Kang-Ho Choia, Ki-Hyun Choa, Juneyoung Leeq, Hee-Joon Bae,c
, Ji Sung Leeb, Beom Joon Kimc, Jong-Moo Parkd, Kyusik Kangd, Soo Joo Leee, Jae Guk Kime, Jae-Kwan Chaf, Dae-Hyun Kimf, Tai Hwan Parkg, Sang-Soon Parkg, Kyung Bok Leeh, Jun Leei, Keun-Sik Hongj, Yong-Jin Choj, Hong-Kyun Parkj, Byung-Chul Leek, Kyung-Ho Yuk, Mi Sun Ohk, Dong-Eog Kiml, Wi-Sun Ryul, Jay Chol Choim, Jee-Hyun Kwonn, Wook-Joo Kimn, Dong-Ick Shino, Sung Il Sohnp, Jeong-Ho Hongp, Man-Seok Parka, Kang-Ho Choia, Ki-Hyun Choa, Juneyoung Leeq, Hee-Joon Bae,c
Dear Sir:
Intravenous tissue plasminogen activator (IV-tPA) is pivotal for the treatment of acute ischemic stroke; however, the benefit of IV-tPA treatment declines rapidly soon after stroke onset [1]. These results support intensive efforts to reduce both onset-to-treatment (OTT) time and door-to-treatment (DTT) time and serve as a basis for establishing an in-hospital and prehospital stroke care system. As these efforts require substantial expenditures of labor and capital, more real-world data are needed to assess the effect of golden hour thrombolysis for acute ischemic stroke. Moreover, understanding the current status and secular changes in IV-tPA treatment will be important to establish an appropriate stroke care system in the future. Therefore, we investigated the effect of golden hour thrombolysis and secular changes in time-to-treatment variables for IV-tPA for acute ischemic stroke by analyzing a prospective registry of 16 stroke centers in South Korea.
This study was based on data from the Clinical Research Collaboration for Stroke in Korea registry of consecutive patients with acute ischemic stroke or transient ischemic attack. From the database, we analyzed the data of patients who were treated with IV-tPA between April 2008 and March 2019. A detailed description of the enrollment process and data collection process is shown in Supplementary Figure 1 and the Supplementary methods. The time metrics, starting from onset or arrival, were defined as follows: (1) onset-to-door (OTD) time was defined as the time from onset (when the patient was last known to be well) to arrival; (2) OTT time was defined as the time from onset to IV-tPA treatment; and (3) DTT time was defined as the time from arrival to IV-tPA treatment. The primary outcome was a good functional outcome at 3 months (a modified Rankin Scale [mRS] score of 0–2). Other outcomes of interest are described in the Supplementary methods.
Multivariable logistic regression models using generalized linear mixed models to account for the effect of hospital (using a random intercept model) were used to explore the relationship between OTT time and the clinical outcome of interest. In addition, we explored the temporal trends in the OTT time, DTT time, and OTD time by calendar year.
A total of 4,248 patients (mean age 67.6±12.6 years; 62% men) were included. In total, 282 (6.6%) patients had an OTT time between 0 and 60 minutes. The general characteristics of patients according to the four OTT windows (0–60, 61–120, 121–180, and 181–270 minutes) are shown in Supplementary Table 1. The associations of OTT windows (as binary, categorical, and continuous variables) with outcomes are shown in Table 1 and Supplementary Table 2. Patients treated within 60 minutes of onset were associated with 35% higher odds of achieving good outcomes at 3 months than those treated beyond 60 minutes of onset (adjusted odds ratio [aOR], 1.35; 95% confidence interval [CI], 1.01 to 1.81). In addition, for every 30-minute delay in treatment, a favorable mRS shift was less likely to occur (OR, 0.93; 95% CI, 0.90 to 0.95) (Supplementary Figure 2).
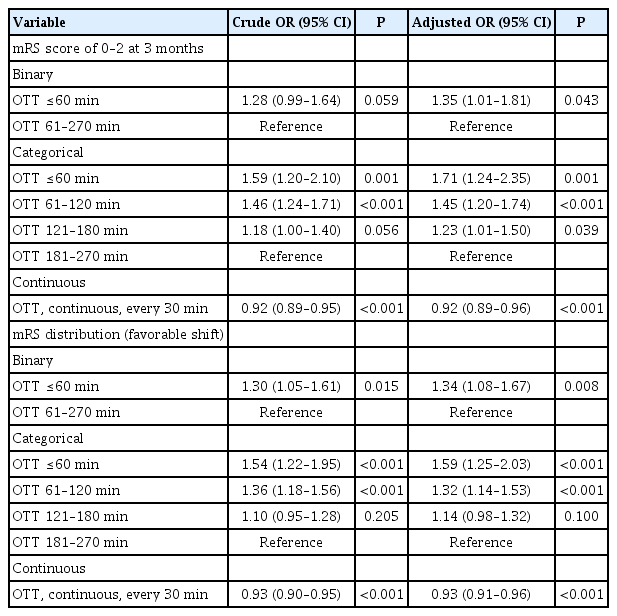
Association of OTT time with functional outcomes at 3 months
From April 2008 to March 2019, the proportion of IV-tPA times within the golden hour increased modestly over time, from less than 6.9% in 2009 to 8.8% in 2019, with associations of 12% higher odds for golden hour thrombolysis for every 1-year increase (aOR, 1.12; 95% CI, 1.03 to 1.21; P=0.005) (Figure 1 and Supplementary Table 3).
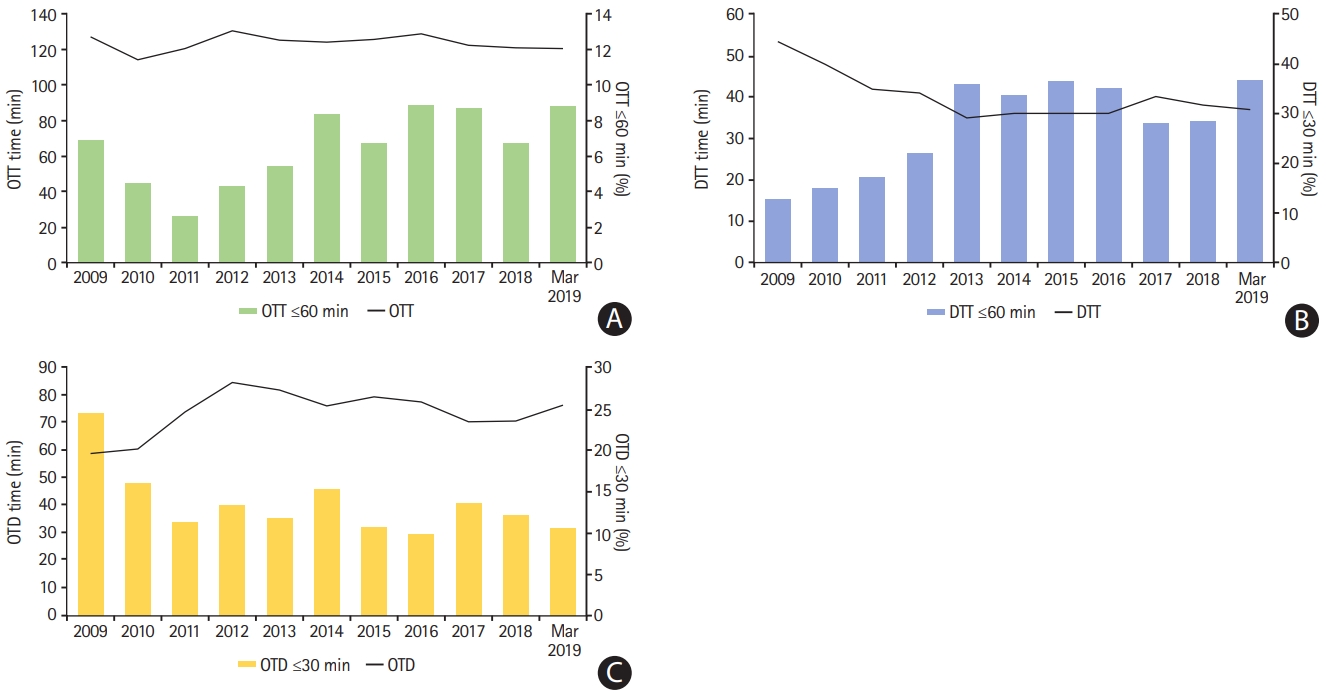
Annual changes in intravenous tissue plasminogen activator treatment times. (A) Onset-to-treatment (OTT) time and the proportions of OTT times ≤60 minutes; (B) door-to-treatment (DTT) time and the proportions of DTT times ≤30 minutes; and (C) onset-to-door (OTD) time and the proportions of OTD times ≤30 minutes.
In an analysis of over 4,200 patients treated with IV-tPA from a nationwide multicenter stroke registry in South Korea, golden hour thrombolysis was associated with better functional outcomes at 3 months than later treatment. The risk of death or symptomatic intracerebral hemorrhage was not associated with golden hour thrombolysis. Time to IV-tPA treatment is an important determinant of 90-day functional outcomes in acute ischemic stroke [2]. In previous studies, golden hour thrombolysis was associated with a good functional outcome at discharge and 3 months [1,3]. Therefore, our study supports the previous results on the effects of golden hour thrombolysis in real-world practice.
In addition, we found that annual rates of golden hour thrombolysis have substantially increased since 2009. These results seemed to be related to the decrease in DTT time or the increasing percentages of DTT time within 30 minutes. Efforts to reduce DTT are the main goal of stroke, and our results support the hypothesis that stroke centers implementing quality improvement programs for in-hospital stroke care improve the workflow of tPA treatment [4-7]. Unlike the results of DTT reduction, the proportion of patients with OTD <30 minutes decreased from that in 2009. This might be an unsolved problem in the stroke system in Korea, and further study is warranted.
This study has several limitations. First, the participating centers did not use uniform guidelines for diagnostic evaluation, patient selection, or IV-tPA treatment workflows. Additionally, detailed hospital factors such as door-to-imaging time were not considered in the analyses. Third, we did not include patients who underwent endovascular thrombectomy. As they might have increased stroke severity, this exclusion could have affected the results. Fourth, our statistical adjustments for patient differences may have been incomplete because of residual or unmeasured confounding variables.
In conclusion, our results show that golden hour thrombolysis could improve the chances of a good outcome at 3 months. Although the data supporting the improvement in in-hospital delay for IV-tPA treatment are clear, the results also suggest that additional efforts to implement more advanced stroke care systems are warranted to further improve acute stroke care in South Korea.
Supplementary materials
Supplementary materials related to this article can be found online at https://doi.org/10.5853/jos.2020.04658.
Acknowledgements
This study was supported by a grant (BCRI20020) from Chonnam National University Hospital Biomedical Research Institute. This study was supported by funding (2020ER620200#) from the Research of Korea Centers for Disease Control and Prevention.
Notes
The authors have no financial conflicts of interest.