Introduction
Endovascular treatment (EVT) is now a well-established management strategy for patients with anterior circulation stroke (ACS) associated with large vessel occlusion (LVO) [1,2]. In contrast, the benefit of EVT for posterior circulation stroke (PCS) patients remains unclear. A large multicenter prospective registry [3] and recent randomized-controlled studies [4,5] did not clearly show the superiority of EVT over medical treatment. In clinical practice, however, EVT is occasionally performed in PCS patients based on observational studies that reported the benefits of EVT [6,7].
For PCS patients, the investigation of clinical characteristics and prognostic factors related to favorable clinical outcomes is important because careful patient selection is required. Predictors of prognosis [8], including the effects of etiology [9-11] have been investigated in ACS patients who underwent EVT. However, although previous studies explored prognostic factors after EVT in PCS patients [12-14], the effects of etiology on clinical outcomes remain uncertain [15-17] and whether the effect is similar or different from ACS counterparts is unknown.
In this study, we investigated differences in clinical outcomes according to etiology in PCS patients who received EVT in comparison with ACS patients. We also compared factors related to favorable outcomes in PCS and ACS patients.
Methods
Patient selection and grouping
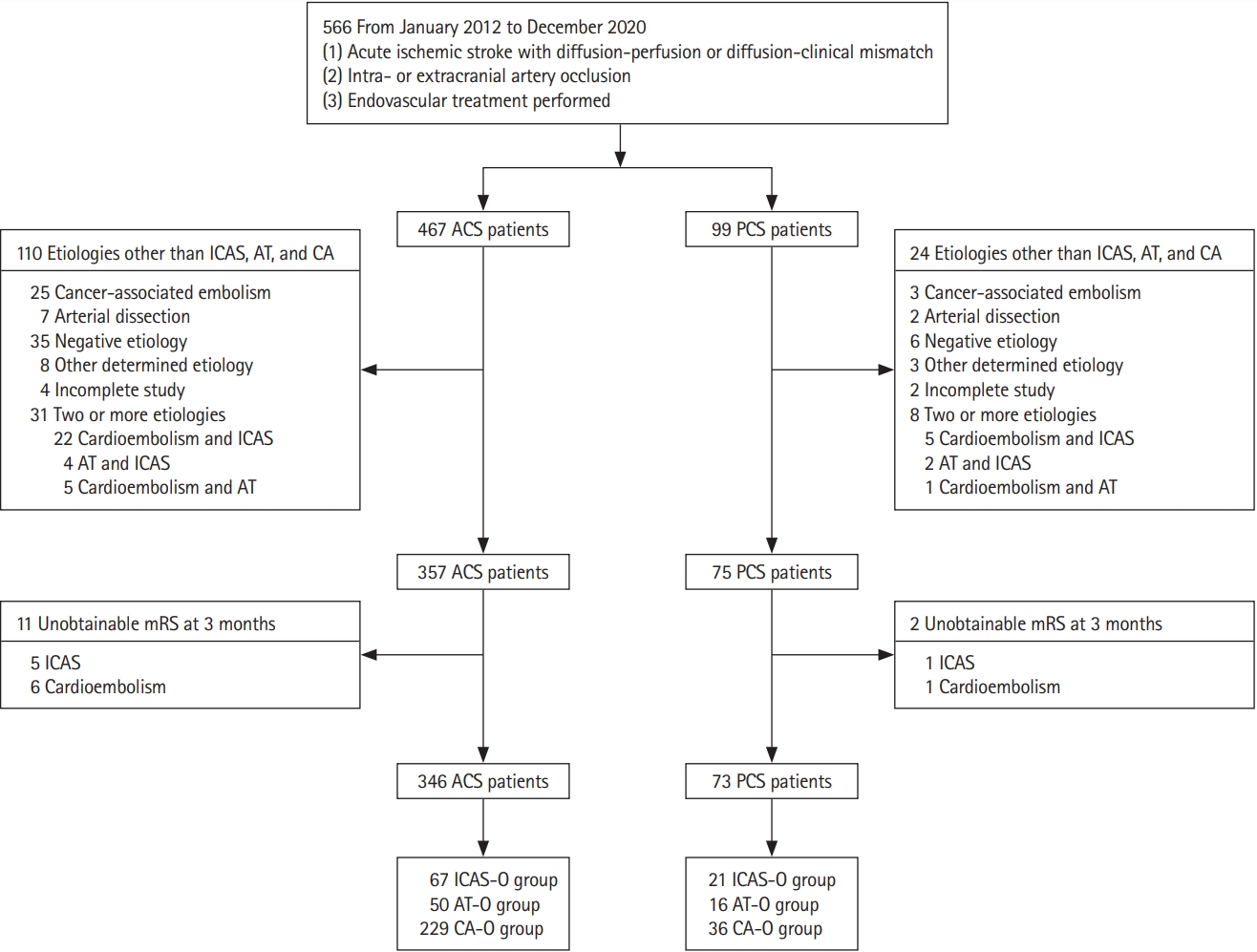
Consecutive patients with acute ischemic stroke (AIS) who underwent EVT between January 2012 and December 2020 at the Asan Medical Center, Seoul, Korea, were prospectively registered. Patients were excluded if (1) they had uncommon etiologies (e.g., arterial dissection, Moyamoya disease, or vasculitis); (2) they had two or more possible etiologies; and (3) their modified Rankin Score (mRS) at 3 months was unobtainable. Enrolled patients were classified as PCS when relevant LVO was found in the vertebral artery (VA), basilar artery (BA), or posterior cerebral artery (PCA).
Patients’ baseline demographic and clinical characteristics, procedural times, National Institutes of Health Stroke Scale (NIHSS) scores, and imaging parameters were obtained from the registry. Stroke etiologies were categorized into intracranial arterial steno-occlusion (ICAS-O), artery-to-artery embolic occlusion (AT-O), and cardioembolic occlusion (CA-O) [18].
ICAS-O was defined when: (1) residual stenosis >70% in the target artery after thrombectomy; (2) moderate stenosis with flow and perfusion impairment on angiography or an evident tendency toward reocclusion; and (3) no source of embolism (e.g., significant proximal arterial stenosis or cardiac disease). Warfarin-Aspirin Symptomatic Intracranial Disease criteria were used to measure the degree of stenosis. AT-O was defined as follows: (1) >50% stenosis in the proximal artery (VA [V1-3 segment], BA, internal carotid artery, common carotid artery [up to the levels of C1], or severe atherosclerosis of the aorta, defined as the presence of atheroma at the aortic arch more than 4 mm in size, detected by transesophageal echocardiography or computed tomography [CT] angiography) associated with relevant, distal artery occlusion associated with relevant, distal artery occlusion, and (2) absence of a cardioembolic source. CA-O was defined when the cardiac disease of medium to high risk of stroke was present, defined by the Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification [19].
The occlusion site was further classified as: extracranial VA (from the origin of the VA to the end of the V3 segment), intracranial VA (from the V4 segment to just before the vertebrobasilar junction), proximal BA (from the level of the vertebrobasilar junction to the anterior inferior cerebellar artery [AICA]), middle BA (from the AICA to the superior cerebellar artery [SCA]), and distal BA (distal to the SCA) [20].
This study was approved by the Institutional Review Board of the Asan Medical Center (IRB number: 2021-1302) and written informed consent was exempted due to the retrospective nature of the study.
Endovascular treatment
In our institute, both CT and magnetic resonance imaging (MRI) facilities are located adjacent to the emergency department for rapid imaging evaluation of stroke patients. All patients with suspected AIS first underwent CT. When hemorrhage was not observed, intravenous tissue plasminogen activator was administered if it could be given ≤4.5 hours after symptom onset. In the meantime, multi-modal MRI was performed, which included diffusion-weighted, perfusion-weighted, fluid-attenuated inversion recovery, and gradient-echo imaging along with magnetic resonance angiography (MRA). When magnetic resonance examination was not possible for any reason (e.g., implantable cardiac defibrillator, head and neck metal implants), CT perfusion and CT angiography were performed instead.
When LVO with a diffusion-perfusion mismatch, according to visual inspection, or diffusion-clinical mismatch was found, the eligibility of EVT was discussed among attending neurologists and neurointerventionists. Although the time widow for EVT is considered to be <24 hours after symptom onset [2], we occasionally performed EVT at ≥24 hours from symptom onset in selected patients if consensus was met. Two experienced neurointerventionists (D.C.S. and D.H.L.) performed EVTs as described elsewhere [21].
The choice of EVT techniques including direct stenting and/or balloon angioplasty, mechanical disruption, direct aspiration, and a stent retriever was at the discretion of the neurointerventionist. In cases of tandem lesions in AT-O patients, the attending neurointerventionist decided which lesion was to be addressed first (e.g., proximal-to-distal or distal-to-proximal).
Evaluation of clinical and angiographic outcomes
We measured times from symptom onset-to-door, door-togroin, puncture-to-recanalization, and onset-to-recanalization. Successful recanalization was defined as modified thrombolysis in cerebral infarction (mTICI) 2b-3. Reperfusion time was defined as the point of time at which successful recanalization was achieved. We calculated the onset-to-recanalization time and the puncture-to-recanalization time in patients in whom successful recanalization was achieved. At 24 to 48 hours post-procedure, follow-up imagings were obtained by MRI/MRA or CT/CT angiography to assess the hemorrhagic transformation and patency of recanalized vessels.
We used a method described by the European Cooperative Acute Stroke Study I trial for the classification of intracerebral hemorrhage (ICH) [22]. Symptomatic hemorrhage was defined as an increase of 4 points or more in the NIHSS score or an increase of 2 points or more in at least one of the 11 subcategories of NIHSS [23]. mRS at 3 months was obtained by structured telephone interview or at the outpatient clinic by a trained nurse clinical specialist. An mRS score ≤2 was regarded as a favorable clinical outcome.
Statistical analysis
Categorical variables were evaluated using Pearson’s chi-square or Fisher’s exact test as appropriate. Mann-Whitney U test was applied when comparing continuous variables, such as demographic variables, the NIHSS score, laboratory parameters, and procedural time. The Kruskal-Wallis test was used for three-group comparisons, and the Mann-Whitney U test was used for two-group comparisons. We performed multivariable binary logistic regression analysis to find independent factors affecting clinical outcomes. Included variables had a P<0.05 on the preceding univariable analysis. A two-sided P value of 0.05 was used to define statistical significance. Statistical analyses were performed using SPSS version 26.0 (IBM Co., Armonk, NY, USA).
Results
Baseline characteristics and clinical outcomes of the ACS and PCS patients
We evaluated 566 consecutive patients with AIS who underwent EVT between January 2012 and December 2020. After excluding 147 patients according to the exclusion criteria, there were 346 (82.6%) patients in the ACS group and 73 (17.4%) in the PCS group (Figure 1).
As shown in Table 1, patients in the PCS group were younger (median age, 67.0 years vs. 71.0 years, P=0.01) and had less frequent CA-O etiology (49.3% vs. 66.2%, P=0.03). Regarding EVT procedure, door-to-groin time (median 144.0 minutes vs. 178.0 minutes, P<0.01), and onset-to-recanalization time (median 421.0 minutes vs. 628.0 minutes, P=0.01) were longer in the PCS group than in the ACS group. At follow-up imaging, there were numerically more ICHs in the ACS group than in the PCS group (42.1% vs. 30.3%, P=0.08). The proportions of successful recanalization and favorable outcomes at 3 months were similar between the two groups, whereas 3 months mortality was higher in the PCS group than the ACS group (15.1% vs. 6.6%, P=0.02).
Baseline characteristics of ACS and PCS patients according to etiology
Table 2 compared patients’ characteristics and outcomes according to each of three etiologies (ICAS-O, AT-O, CA-O) between the ACS and PCS groups; there were 67 (19.4%), 50 (14.5%), and 229 (66.2%) patients in the ACS group and 21 (28.8%), 16 (21.9%), and 36 (49.3%) patients in the PCS group, respectively. Baseline characteristics were similar between the ACS and PCS groups in each etiology except for a higher proportion of previous stroke history (18.0% vs. 50.0%, P=0.02) of AT-O patients in the PCS group.
Procedural and clinical outcomes of ACS and PCS patients according to etiology
EVT procedure-related time variables, including onset-to-door and onset-to-recanalization times were not significantly different between the ACS and PCS groups in ICAS-O and AT-O patients (Table 2). However, among CA-O patients, the PCS group had longer door-to-groin puncture time (median 179.0 minutes vs. 132.0 minutes, P<0.01) than the ACS group, whereas puncture-to-recanalization time (median 36.5 minutes vs. 51.0 minutes, P<0.01) was shorter in the PCS group than in the ACS group. The use of EVT modalities and proportion of successful recanalization (mTICI 2b-3), as well as favorable 3-month clinical outcomes, were similar in all three etiologies between the ACS and PCS groups (Table 2 and Figure 2).
Baseline characteristics, and procedural and clinical outcomes of ACS patients according to etiology
We also analyzed the baseline characteristics and outcomes of patients according to etiology, confined to each ACS and PCS group. The results of ACS patients are summarized in Supplementary Table 1. The median age (ICAS-O, 65.5 years; AT-O, 68.5 years; CA-O, 74.0 years; P<0.01) and proportion of female sex (ICAS-O, 19.4%; AT-O, 12.0%; CA-O, 51.1%; P<0.01) were higher in the CA-O group. The initial NIHSS score was higher in the CA-O group (ICAS-O, 9.0; AT-O, 10.0; CA-O, 14.0; P<0.01). Procedural variables showed that CA-O patients had a shorter time interval in all aspects, including onset-to-door (ICAS-O, 505.0 minutes; AT-O, 274.0 minutes; CA-O, 120.0 minutes; P<0.01), door-to-puncture (ICAS-O, 212.0 minutes; AT-O, 156.5 minutes; CA-O, 132.0 minutes; P<0.01), and onset-to-recanalization time (ICAS-O, 950.0 minutes; AT-O, 559.5 minutes; CA-O, 346.0 minutes; P<0.01). The rate of successful recanalization, favorable clinical outcome, and mortality at 3 months were similar among the three etiologies.
Baseline characteristics, and procedural and clinical outcomes of PCS patients according to etiology
Among PCS group patients, the median age and initial NIHSS score were not significantly different, but female sex was more frequent in the CA-O group (ICAS-O, 14.3%; AT-O, 12.5%; CA-O, 55.6%; P<0.01) (Supplementary Table 2). Analysis of procedural time variables showed that onset-to-door and door-to-puncture times were similar among the three etiologies, whereas puncture-to-recanalization time (ICAS-O, 72.0 minutes; AT-O, 62.0 minutes; CA-O, 36.5 minutes; P<0.01) and onset-to-recanalization time (ICAS-O, 659.0 minutes; AT-O, 973.0 minutes; CA-O, 511.5 minutes; P=0.04) was the shortest in CA-O patients. The rate of TICI 2b-3, 3-month mRS 0-2, and 3-month mortality were similar among the three etiologies.
Factors related to favorable clinical outcomes
Univariable analysis showed that age, baseline NIHSS score, and ICH at follow-up imaging for the PCS group, and age, baseline NIHSS score, successful recanalization, and ICH at follow-up imaging for the ACS group were associated with clinical outcomes (Table 3). Multivariable analysis showed that baseline NIHSS score (odds ratio [OR], 0.84; 95% confidence interval [CI], 0.75 to 0.93; P=0.001) and ICH at follow-up imaging (OR, 0.20; 95% CI, 0.04 to 0.97; P=0.046) in the PCS group, and baseline NIHSS score (OR, 0.86; 95% CI, 0.81 to 0.91; P<0.001), successful recanalization (OR, 11.74; 95% CI, 2.60 to 52.94; P=0.001), and ICH at follow-up imaging (OR, 0.47; 95% CI, 0.29 to 0.77; P=0.003) in the ACS group were independently associated with favorable 3-month mRS scores.
Discussion
In this study, we compared EVT procedure and clinical outcomes between the PCS and ACS groups, focusing on three etiologies, ICAS-O, AT-O, and CA-O. We found that PCS group patients were younger, had less frequent CA-O etiology, and longer onset-to-recanalization time and door-to-puncture time than ACS group patients. The proportions of successful recanalization and favorable clinical outcomes at 3 months were similar among the three etiologies between the ACS and PCS groups.
The onset-to-recanalization time, which is the sum of onset-to-door, door-to-puncture, and puncture-to-recanalization time, was longer in PCS patients than in ACS patients. As shown in Table 1, the difference mainly resulted from the longer onset-to-door and door-to-puncture times in PCS patients. The relatively longer onset-to-door time in the PCS group was probably attributed to symptoms such as dizziness, diplopia, visual dimness, or dysphagia, which were not regarded as serious neurologic symptoms by the patients. Although the reason for delayed door-to-puncture time in PCS patients is less clear, further analysis showed that the difference was obvious only in the CA-O patients (Table 2). Thus, the difference was in part related with different characteristics of CA-O between the PCS and ACS groups. Although the NIHSS score was highest in CA-O patients in the ACS group (Supplementary Table 1), it was similar among the three etiologies in the PCS group (Supplementary Table 2). This is probably due to the different symptom characteristics of CA-O patients between the two groups. Although CA-O in the ACS group produced abrupt and severe motor dysfunction associated with sudden middle cerebral artery or internal carotid occlusion (Supplementary Table 1), CA-O in the PCS group typically occluded distal basilar or PCAs [24-26] (Supplementary Table 2), which is less likely to produce severe motor dysfunction, thereby delaying the initiation of the EVT decision.
Interestingly, in the CA-O patients, puncture-to-recanalization was shorter in the PCS group than in the ACS group (Table 2). The reason remains unclear. Perhaps, in CA-O patients without proximal artery atherosclerosis, access to the occluded thrombi may be relatively difficult in ACS patients due to the presence of curved carotid syphons. Morphological anomalies such as tortuosity or coiling has been reported to common in the internal carotid artery [27]. Alternatively, the presence of the collateral flow of the posterior circulation, such as the posterior communicating arteries and superficial anastomosis [28], might have a role in spontaneous thrombus fragmentation. These anatomic characteristics may also partly explain why the proportion of favorable clinical outcomes was similar despite the relatively prolonged onset-to-recanalization time in the PCS group when compared with the ACS group (Table 2).
Among patients with embolic occlusion, we separated AT-O from CA-O. The efficacy and safety of EVT in tandem lesions in ACS patients have been described [29,30]. However, the appropriate treatment of tandem occlusion in PCS patients still needs to be investigated, although a considerable proportion of PCS patients receiving EVT are classified into this group [31-33]. In our study, the proportion of successful recanalization as well as 3-month favorable clinical outcomes in AT-O patients in the PCS group were all comparable with those of AT-O patients in the ACS group (Table 2), suggesting the efficacy and safety of EVT in this group of patients.
After the multivariable analysis, low baseline NIHSS score and the absence of cerebral hemorrhage were significantly related to favorable outcomes in PCS and ACS patients, whereas successful recanalization was an independent factor for ACS patients only. Previous studies found that PCS patients with EVT had a lower rate of functional independence despite a rate of successful recanalization similar to that of ACS patients [34,35]. This might be explained by a higher proportion of futile reperfusions in PCS compared to ACS, as previously suggested [34]. In addition, mRS score, which is a widely used scoring system to evaluate clinical outcomes, might not be an appropriate tool for PCS patients, because symptoms such as visual field defect, dizziness, ataxia, and paresthesia are not properly reflected in this scoring system [36]. Thus, the possible benefit of recanalization therapy may have been underestimated in studies using mRS as an outcome parameter.
There were several limitations in this study. First, because this was a single center, retrospective study, there may have been selection bias. Second, as the number of PCS patients was relatively small, although it was comparable to previously published studies [14,25]. Third, an assessment of collaterals was not systemically performed in this retrospective study. Lastly, patients with missing 3-month mRS were excluded from this study, which may introduced a selection bias.
Conclusions
In this study, we found that PCS group patients, especially in the CA-O group, had longer door-to-puncture and onset-to-recanalization times although favorable clinical outcomes were similar in the ACS and PCS groups, regardless of etiology. The lower baseline NIHSS score and the absence of hemorrhagic transformation were related to favorable outcomes in PCS patients, but not successful reperfusion, which was related to favorable outcomes in ACS patients. More studies are needed to examine the role of EVT in PCS patients.