Explanatory Power and Prognostic Implications of Factors Associated with Troponin Elevation in Acute Ischemic Stroke
Article information

Abstract
Background and Purpose
We investigated the impact of comorbidity burden on troponin elevation, with separate consideration of neurological conditions, in patients with acute ischemic stroke (AIS).
Methods
This prospective, observational cohort study consecutively enrolled patients with AIS for 2 years. Serum cardiac troponin I was repeatedly measured, and disease-related biomarkers were collected for diagnosis of preassigned comorbidities, including atrial fibrillation (AF), ischemic heart disease (IHD), myocardial hypertrophy (MH), heart failure (HF), renal insufficiency (RI), and active cancer. The severity of neurological deficits and insular cortical ischemic lesions were assessed as neurological conditions. Adjusted associations between these factors and troponin elevation were determined using a multivariate ordinal logistic regression model and area under the receiver operating characteristic curve (AUC). Cox proportional hazards model was used to determine the prognostic significance of comorbidity beyond neurological conditions.
Results
Among 1,092 patients (66.5±12.4 years, 63.3% male), 145 (13.3%) and 335 (30.7%) had elevated (≥0.040 ng/mL) and minimally-elevated (0.040–0.010 ng/mL) troponin, respectively. In the adjusted analysis, AF, MH, HF, RI, active cancer, and neurological deficits were associated with troponin elevation. The multivariate model with six comorbidities and two neurological conditions exhibited an AUC of 0.729 (95% confidence interval [CI], 0.698–0.759). In Cox regression, AF, IHD, and HF were associated with adverse cardio-cerebrovascular events, whereas HF and active cancer were associated with mortality.
Conclusion
Troponin elevation in patients with AIS can be explained by the burden of comorbidities in combination with neurological status, which explains the prognostic significance of troponin assay.
Introduction
Cardiac troponins are structural proteins of cardiomyocytes, and elevated serum troponin levels indicate myocardial injury. Thus, troponin elevation, especially above the 99th percentile of the upper reference limit (URL), has been used as a diagnostic and prognostic biomarker in acute coronary syndrome (ACS) [1]. Furthermore, the use of the troponin assay has expanded the risk stratification in various patients, including those with stroke, stable coronary artery disease (CAD), atrial fibrillation (AF), heart failure (HF), myocardial hypertrophy (MH), renal insufficiency (RI), and even in the general population [2].
However, the interpretative strategy of troponin elevation remains unclear [3], especially in patients with acute ischemic stroke (AIS), owing to its complexity [4]. Patients with AIS frequently have various cardiac comorbidities, which can contribute to troponin elevation [5]. Furthermore, patients with AIS are mostly older adults and often have multiple comorbidities, including cardiac and non-cardiac comorbidities, which also contribute to troponin elevation, apart from the troponin elevation through neurogenic stress [6]. Thus, although international guidelines for AIS management recommend the measurement of the baseline troponin level in conjunction with electrocardiography (ECG) in all patients [7], the practical application of the troponin assay is only available to assess a few specific conditions, such as concurrent ACS and cardiac arrhythmia, without a strategic approach.
Therefore, this study aimed to evaluate the influence of comorbidity burden on troponin elevation and prognostic significance, with separate consideration of neurological conditions in patients with AIS.
Methods
Study population
This study is a registered, prospectively enrolled, and observational study designed to investigate the prognostic significance [8] and the possible mechanisms of troponin elevation for enhancing the practical application of troponin measurement in patients with AIS (Clinical Research Information Service [CRIS]; KCT0000682; https://cris.nih.go.kr/cris).
All consecutive patients with AIS who visited the emergency room within 48 hours after the onset of acute neurological deficit at the Asan Medical Center in Korea between March 2013 and March 2015 were prospectively recruited. On admission, patients with suspected ACS were evaluated by cardiologists to determine the urgency of coronary angiographic assessment and excluded from this study. The Institutional Review Board of the Asan Medical Center approved this study (IRB no. 2012-0561). Informed consent was obtained from each patient or their legal delegates.
Study protocol
Figure 1 shows the flow diagram of the study protocol. Registered patients routinely underwent measurements of serum cardiac troponin I level. The troponin level on the second day after stroke onset was designated as the reference value, considering the dynamic features of troponin release. The lower limit of detection of serum cardiac troponin I was 0.006 ng/mL, and the calculated 99th percentile of the URL was 0.040 ng/mL (Abbott Laboratories, Abbott Park, IL, USA). The patients were categorized into three groups: (1) troponin I level ≥0.040 ng/mL was defined as “elevated,” (2) troponin I level between 0.040 and 0.010 ng/mL was interpreted as “minimally-elevated,” and (3) troponin I level <0.010 ng/mL was defined as “non-detectable troponin.” [8]

Flow diagram of the study protocol. Process of patient selection and classification according to the troponin level and diagnosis of troponin elevation-related factors to assess their predictive value. AIS, acute ischemic stroke; ECG, electrocardiography; BNP, b-type natriuretic peptide; NIHSS, National Institutes of Health Stroke Scale; AF, atrial fibrillation; IHD, ischemic heart disease; MH, myocardial hypertrophy; HF, heart failure; RI, renal insufficiency; MACCE, major adverse cardiac and cerebrovascular event.
Based on prior research [9,10], the disease-related biomarkers were prospectively collected to improve the diagnostic accuracy of troponin elevation-related comorbidities: (1) repeated 12-lead ECG (GE Healthcare, Waukesha, WI, USA), with the results processed using the Marquette 12SL ECG analysis program; (2) serum b-type natriuretic peptide (BNP) level measured on day 2 after stroke onset and repeated if patients had a borderline BNP elevation (i.e., >200 or >100 pg/mL in patients with or without RI, respectively) [11]; (3) estimated glomerular filtration rate (GFR) at admission; and (4) serum D-dimer and fibrinogen at admission to assess coagulopathy, considering screening for cancer-related coagulopathy [12], or pulmonary embolism.
Data collection
Clinical data, including demographic characteristics, conventional vascular risk factors, and laboratory data, were obtained. The preassigned comorbidities were defined based on the parameters of disease-related biomarkers, historical information, or both, as follows: (1) AF in the known history or positive on serial ECGs at least once; (2) ischemic heart disease (IHD) in the known history or positive ischemic-ECG changes (e.g., ST-segment elevation or depression, T-wave inversion, left bundle branch block [LBBB], or pathological Q-waves) on serial ECGs at least once; (3) MH in the known history or positive ventricular hypertrophy (VH) on serial ECGs at least once; (4) HF in the known history or an elevated BNP >500 pg/mL on serial measurements of BNP; (5) RI in the known history or an impaired GFR (<60 mL/min/1.73 m2, calculated using the Modification of Diet in Renal Disease formula); and (6) active cancer (e.g., cancer within six months before enrollment, any treatment for cancer within the previous six months or recurrent or metastatic cancer, or newly diagnosed cancer after stroke). The stroke severity was assessed using the National Institutes of Health Stroke Scale (NIHSS) [13] score to define troponin elevation-related neurological factors, and the specific ischemic lesion location on the insular cortex was assessed on a diffusion-weighted magnetic resonance image [14]. Reperfusion therapy was defined as intravenous tissue plasminogen activator or intra-arterial reperfusion therapy, or both.
Follow-up information was obtained via a direct interview at the outpatient department or a telephone interview by the research coordinator, including major adverse cardiac and cerebrovascular events (MACCE, any cardiac or cerebrovascular death, nonfatal ACS, ischemic or hemorrhagic stroke, and coronary revascularization) and all causes of death to assess the long-term prognostic value.
Substudy for assessment of subclinical ACS risk
Considering underdetection of subclinical ACS risk, multidetector coronary computed tomography angiography (CTA) was prospectively performed for selected patients in the elevated, minimally-elevated, and non-detectable groups at a 1:2:2 ratio, after the exclusion of patients who were diagnosed with RI or those in whom performing coronary CTA was difficult (e.g., altered mental status, language dysfunction, and unstable medical conditions). CTA was performed using a dual-source scanner (SOMATOM Definition, Siemens, Erlangen, Germany), and 400 mg/mL iodine (Iomeron 400, Bracco, Milan, Italy) was used. According to the guidelines, a 16-segment coronary artery tree model was used.
Furthermore, the possible etiology of high-risk patients with a troponin surge (>1.00 ng/mL, indicating extensive myocardial injury highly related to ACS) was assessed.
Statistical analysis
Baseline characteristics between the troponin I categories were compared using the chi-square test for categorical variables. Continuous variables were compared using Student’s t-test or analysis of variance with Duncan’s post hoc correction. To describe the influence of individual factors on troponin elevation (both elevated and minimally-elevated troponin levels), we obtained the odds ratio (OR) by multivariate ordinal logistic regression analysis using backward elimination (likelihood ratio test). Furthermore, to explore the integrated impact of the factors on troponin elevation, we incorporated them into the models in four ways to estimate the area under the receiver operating characteristic curve (AUC) for predicting troponin elevation: (1) six comorbidities; (2) six comorbidities and two neurological factors; (3) all independent factors related to troponin elevation besides the eight main variables; and (4) all variables in Table 1 except for reperfusion therapy.

Baseline characteristics according to the troponin value
After adjusting for all variables in Table 1 and the reference troponin value, the multivariate Cox proportional hazard model was used to determine the predictive value of individual comorbidity for long-term risk of MACCE and mortality. The results of the Cox analysis were reported as a hazard ratio (HR) and 95% confidence interval (CI). Statistical analysis was performed using the Statistical Package for the Social Sciences (version 17.0; SPSS Inc., Chicago, IL, USA).
Results
General characteristics
The mean age of 1,092 consecutive patients with AIS over 2 years was 66.5±12.4 years (range, 18–95 years), and 691 patients (63.3%) were men. The overall distribution of serum troponin levels peaked on day 2 after stroke onset, and almost half of patients with elevated (43.5%) and minimally-elevated (49.9%) troponin had newly detected troponin elevations compared to the baseline level (Supplementary Figure 1A and B).
A total of 480 (44.0%) patients had troponin elevation; 145 (13.3%) had elevated and 335 (30.7%) had minimally-elevated troponin. Patients with troponin elevation were older and had a higher prevalence of hypertension and diabetes but a lower prevalence of smoking than those with non-detectable troponin levels. Moreover, these patients had a higher prevalence of comorbidities, a higher severity of neurological deficits, and a higher prevalence of insular cortical lesions than those with non-detectable troponin levels. They received more reperfusion treatment than those with non-detectable troponin levels. Moreover, patients with troponin elevation showed a higher leukocyte count and higher glucose, homocysteine, C-reactive protein, and total bilirubin levels but lower hemoglobin, platelet, low-density lipoprotein, albumin, and total protein levels than those with non-detectable troponin levels (Table 1).
Influence of troponin elevation-related factors
Multivariate ordinal logistic regression analyses were performed to determine the contribution of individual factors to troponin elevation (Table 2). The comorbidities, including AF (OR, 1.41; 95% CI, 1.05–1.89), MH (OR, 1.97; 95% CI, 1.48–2.63), HF (OR, 2.65; 95% CI, 1.64–4.27), RI (OR, 1.89; 95% CI, 1.37–2.59), active cancer (OR, 1.92; 95% CI, 1.17–3.14), and neurological status such as NIHSS score (OR, 1.05; 95% CI, 1.02–1.07) were associated with troponin elevation. In addition, IHD and insular lesions tended to be related to troponin elevation. Moreover, age (OR, 1.04; 95% CI, 1.02–1.05 per 1-year increase), leukocyte count (OR, 1.10; 95% CI, 1.05–1.16), platelet count (OR, 0.96; 95% CI, 0.95–0.98), and albumin level (OR, 0.50; 95% CI, 0.36–0.70) were associated with troponin elevation.

Ordinal logistic regression analysis of the contribution of factors related to troponin elevation along with elevated and minimally-elevated troponin levels
Model 1, with six comorbidities, showed an AUC of 0.715 (95% CI, 0.684–0.745) for predicting troponin elevation. The accuracy of a diagnostic test for predicting troponin elevation was further improved to an AUC of 0.729 (95% CI, 0.698–0.759) after including two neurological factors on top of Model 1. Additionally, the estimated AUC of 0.772 (95% CI, 0.744–0.800) after the inclusion of other independent troponin elevation factors on top of model 2 was comparable to that of the final model with an AUC of 0.778 (95% CI, 0.749–0.806) (Table 3).
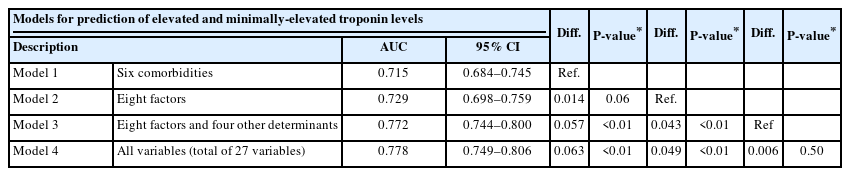
An AUC and goodness-of-fit test for the multivariate models for predicting troponin elevation
Prognostic value of troponin elevation-related factors
During a median follow-up of 18 months (interquartile range, 11–26 months), 179 (17.0%) patients experienced MACCE, and 132 (12.1%) died. The Cox proportional hazards analysis showed that AF (HR, 1.49; 95% CI, 1.05–2.10), IHD (HR, 1.54; 95% CI, 1.09–2.17), and HF (HR, 1.91; 95% CI, 1.24–2.93) are associated with increased risk of MACCE, and HF (HR, 1.73; 95% CI, 1.07–2.80) and active cancer (HR, 2.86; 95% CI, 1.69–4.83) with increased risk of all causes of death. In addition, IHD and MH were associated with an increased risk of all causes of death (Table 4).

Unadjusted and adjusted HR for the individual contribution of comorbidities to clinical outcomes during the 3-year follow-up
Substudy for assessment of subclinical ACS risk
Among the 142 enrolled patients, no significant difference in the degree or number of CAD across the different troponin levels was observed. Almost half of the patients had no significant CAD, regardless of the troponin level (Table 5).

Coronary CTA according to troponin level
Only nine of the 29 patients with troponin surge (2.7%) were presumed to have symptomatic CAD (six cases with ACS and three cases with recent angina within 7 days). Among the remaining 20 patients, stress-induced cardiomyopathy (SICMP; six patients were in a comatose state, n=7), active cancer with extensive multiple metastases (all patients had D-dimer levels >25 μg/mL, n=5), and other medical conditions (n=8) were suspected as primary causes of troponin surge (Supplementary Table 1).
Discussion
This prospective study verified the overall influence of comorbidity burden on troponin elevation in AIS, with separate consideration of neurological status. In this study, the overall incidence of troponin elevation was not comparable with that observed in previous studies because our unique time point defined the troponin level two days after stroke onset as the reference level. Traditionally, the guidelines for AIS management recommend repeated troponin measurements in a few cases with the possibility of development of silent ischemia [7]. However, assessing dynamic changes in troponin levels is still important for differentiating the cause of cardiomyocyte damage and distinguishing acute elevations from chronic ones that are associated with a variety of chronic conditions [1], which can be further clarified using a highly sensitive troponin assay for the deliberate detection of dynamic change [3]. In this context, our study shows that repeated troponin measurements using a highly sensitive troponin assay can enhance the detection and tracking of troponin elevation, including newly detected as well as minimally-elevated troponin (Supplementary Figure 1A and B), and the risk stratification power to detect more high-risk patients with a higher burden of comorbidity and neurological deficits (Supplementary Figure 1C and D).
We verified the individual influence of six comorbidities on troponin elevation (Table 2), and their integrated influence on troponin elevation in combination with two neurological factors showed an AUC of 0.729 (Table 3). Therefore, troponin elevation in AIS can be explained by the burden of comorbidities in combination with neurological status, which, in turn, explains the prognostic value of the troponin assay in these patients when the prognostic significance of each comorbidity beyond neurological status is considered (Table 4). Troponin elevation indicates underlying cardiac comorbidities, which leads to an increased risk of cardiogenic embolic stroke with extensive ischemic lesions [15]. Furthermore, apart from the fatal impact of stroke, underlying comorbidities (i.e., AF [16], HF [17], IHD [18], MH [19], and RI [20]) also lead to poor outcomes. Therefore, despite the skeptical viewpoint on intensive cardiac monitoring in the recent AIS guidelines [7], detecting troponin elevation-related comorbidities by measuring disease-related biomarkers can be a complementary tool for long-term risk stratification in patients with AIS.
In this study, the detection of subclinical ACS risk remains a diagnostic challenge, considering its fatal outcome. Patients with AIS are often older adults, and concomitant cardiac pathology is common; however, acquiring ACS symptoms is difficult due to cognitive dysfunction, aging, or neurological deficits. Thus, we attempted to define IHD based on the ischemic-ECG findings apart from the patients’ medical history because elevated troponin levels caused by “silent ischemia” can be monitored using ischemic-ECG changes [21]. Finally, the overall IHD incidence (25.3%) was consistent with that reported in the literature (e.g., 20%–30% and 40% for symptomatic and asymptomatic IHD, respectively) [22]. Additionally, among the 142 randomly selected patients, coronary CTA revealed no significant difference in grade or number of CAD across different troponin levels; half of the patients had no CAD (Table 5). This finding corroborates with those of a previous study that showed less frequent coronary culprit lesions in patients with AIS than in age- and sex-matched controls with non-ST-segment elevation myocardial infarction (NSTEMI), despite similar baseline troponin levels [23]. Furthermore, of the 29 patients with a troponin surge, only nine were presumed to have symptomatic CAD (Supplementary Table 1). Therefore, troponin elevation indicates a burden of various ranges of cardiac and non-cardiac comorbidities in patients with AIS, even when subclinical ACS risk is considered.
Previously, we suggested the cerebrogenic myocardial injury (CMI) concept to explain the troponin elevation in AIS and could confirm it in this study (Supplementary Figure 2): synergistic interaction between vulnerable cardiac status (e.g., hypertrophic or damaged myocardium) and specific neurological conditions, leading to troponin elevation [10]. Finally, we proposed a diagnostic approach model for improving the practical application of the troponin assay in patients with AIS: (1) serial troponin measurements can improve the detection and tracking of the troponin level considering newly detected troponin elevation; (2) measurements of disease-related biomarkers can improve the detection of comorbidities, with the merit of long-term prognostic value beyond stroke severity; and (3) separate recognition of neurological status can show the interactive influence of neurogenic stress on comorbidity burden (Figure 2). Hence, stroke should be considered a systemic disease, and bidirectional interactions between the brain and peripheral organs should be considered for comprehensive therapeutics for AIS [4].

Diagnostic approach model for assessing troponin elevation in patients with AIS. Process for detecting the troponin elevation (red line) and etiological evaluation of troponin elevation (blue line), including the recommendation of the clinical process (blue box) and diagnosis of the troponin elevation-related factors (green box). AIS, acute ischemic stroke; CMI, cerebrogenic myocardial injury; NIHSS, National Institutes of Health Stroke Scale; ECG, electrocardiography; ACS, acute coronary syndrome; STEMI, ST-segment elevation myocardial infarction; NSTEMI, non-ST-segment elevation myocardial infarction; RI, renal insufficiency; SICMP, stress-induced cardiomyopathy; AF, atrial fibrillation; IHD, ischemic heart disease; MH, myocardial hypertrophy; HF, heart failure; RI, renal insufficiency; CT, computed tomography; LBBB, left bundle branch block. *ECG pattern, including (1) suspicious STEMI, which initially developed as an acute ischemic change (e.g., ST-segment elevation or LBBB), followed by newly developed Q-wave on serial ECG investigation; and (2) suspicious NSTEMI, which transiently/persistently developed as an acute ischemic change (e.g., ST-segment depression with or without T-wave inversion) on serial ECG investigation.
Study limitations
This study has several limitations. First, this study was conducted at a single center; all patients were Asian. Second, the diagnostic accuracy of comorbidities based on disease-related biomarkers might remain limited; ischemic-ECG alone is often insufficient to diagnose IHD because it depends on various CAD conditions (e.g., size, arterial segment distribution, collateral vessels, location, extent, coronary stenosis severity, and prior myocardial necrosis) and may be observed in other conditions (e.g., acute pericarditis, VH, LBBB, the Brugada syndrome, SICMP, and early repolarization patterns) [21]. HF diagnosis was difficult owing to limited diagnostic values, and the main terminology was based on the left ventricle ejection fraction measurement. ECG diagnostics of VH are based on the QRS voltage criteria for diagnosing MH; however, an increased QRS voltage in actual anatomical VH is not a consistent finding. Nonetheless, an alternative diagnostic approach in clinical practice includes serum level measurement of BNP as a “rule-out” test in HF diagnosis [24], and the ECG criteria for VH are a strong independent predictor of cardiovascular morbidity and mortality [25]. Furthermore, when we applied more strict criteria for defining cardiac comorbidity based on the echocardiographic findings, such as IHD, MH, and HF [26], the statistical significance of their individual influences on troponin elevation and long-term prognostic value were still preserved, and their overall explanatory power for troponin elevation was further improved (Supplementary Tables 2-4). Third, the findings of coronary CTA have a generalization limitation because we only recruited 25% of eligible patients. However, the main confounders (e.g., age, sex, and prevalence of IHD) for determining the difference in CAD severity were similar across the troponin levels.
Conclusions
The elevation of serum troponin levels in patients with AIS is associated with the increasing burden of troponin elevation-related comorbidities, with a synergistic impact on the neurological status and a proportionally increased risk of long-term adverse outcomes. Thus, serum troponin levels, especially considering dynamic changes along with disease-related biomarkers, can be helpful in the risk stratification of patients with AIS.
Supplementary materials
Supplementary materials related to this article can be found online at https://doi.org/10.5853/jos.2022.02012.
Presumptive diagnoses and outcomes of patients with troponin surge exceeding 1.00 ng/mL
Recalculated ordinal logistic regression analysis of the contribution of factors related to troponin elevation along with elevated and minimally-elevated troponin levels
Redefined area under the ROC curve and goodness-of-fit test of the multivariate models for predicting troponin elevation
Redefined unadjusted and adjusted HRs for the individual contribution of comorbidities to clinical outcomes during the 3-year follow-up
The dynamic pattern of serum troponin levels across time (A and B) and the burden of comorbidity and neurological status according to dynamic changes in categorized troponin levels (C and D). Newly detected troponin elevation (red dotted box) was compared with baseline troponin (blue dotted box) based on the categorized values. The burden of comorbidities was defined as the total number of predefined comorbidities, and the neurological burden as the mean NIHSS score. SD, standard deviation; ET, elevated troponin; MET, minimally-elevated troponin; NDT, non-detectable troponin; CI, confidence interval; NIHSS, National Institutes of Health Stroke Scale. *P<0.05 using analysis of variance with Duncan’s post hoc test.
Influence of comorbidity burden and neurological status on troponin elevation. (A) Comorbidity burden (defined as the total number of candidate comorbidities) and composite neurological conditions (defined as either moderate to severe deficit [NIHSS of ≥7 points], insular lesions, or both) increased linearly as the troponin level increased. (B) Conversely, the magnitude of troponin elevation increased linearly as the comorbidity burden increased, with rates being further higher in patients with a composite neurological status. NIHSS, National Institutes of Health Stroke Scale; N., number; NDT, non-detectable troponin; MET, minimally-elevated troponin; ET, elevated troponin; OR, odds ratio; CI, confidence interval; TC, total comorbidities. *P<0.05 of OR for each number of TC after adjusting for age, sex, conventional risk factors, and all laboratory results; †P<0.05 of OR of a composite neurological factor after adjusting for age, sex, conventional risk factors, all laboratory results, and the number of TC.
Notes
Disclosure
The authors have no financial conflicts of interest.
Acknowledgements
This study was supported by a grant from the National Research Foundation of Korea (NRF-2020R1F1A1073802, S.-H. Ahn), funded by the Korea government (MSIT).