Genotype–Phenotype Correlation of the RNF213 R4810K Variant in Moyamoya Disease
Article information

Dear Sir:
The R4810K variant of ring finger protein 213 (RNF213) was identified as a strong genetic susceptibility factor for moyamoya disease (MMD) in the East Asian population [1,2]. The RNF213 R4810K variant is associated with significantly early age of onset and the severity of clinical disease phenotypes [3-5]. However, its association with various other clinical presentations and long-term patient outcomes has not been fully established [6,7]. This study aimed to investigate the influence of the RNF213 R4810K variant on clinical phenotypes and long-term outcomes in Korean patients with MMD.
This retrospective study involved 311 Korean patients with MMD who had undergone RNF213 genotyping at two tertiary university hospitals between January 2017 and August 2021. A flowchart for the selection of MMD with RNF213 genotyping is shown in Supplementary Figure 1. The detailed methodology is described in the Supplementary Methods. Briefly, clinical manifestations including cerebral infarction, transient ischemic attack (TIA), intracranial hemorrhage/intraventricular hemorrhage (ICH/IVH), seizure, and angiographic characteristics including bilateral vasculopathy, posterior cerebral artery (PCA) involvement, and Suzuki grade were assessed at diagnosis of MMD. The association between the RNF213 R4810K variant and clinical/angiographic characteristics at MMD diagnosis was investigated. Moreover, among patients with at least 3 months of follow-up, we evaluated the influence of the RNF213 R4810K variant on long-term clinical outcomes and the results of revascularization after bypass surgery. This study was reviewed and approved by Severance Hospital Yonsei University Health System Institutional Review Board (3-2021-0443). The requirement for written informed consent was waived due to the retrospective study design.
The clinical and angiographic characteristics of 311 patients with MMD are summarized in Supplementary Table 1. The distribution of age peaked twice—at ages 5–9 and 45–49 years—with a higher frequency in the adult peak (Supplementary Figure 2A). Compared to adult MMD patients, pediatric MMD patients more frequently presented with ischemic manifestations and seizures and had a higher proportion of bilateral vasculopathy. The correlation between clinical characteristics and the RNF213 R4810K variant in MMD is summarized in Table 1 and Supplementary Figure 3. The age at onset of homozygotes was significantly lower than those of heterozygotes and the wild-type (Supplementary Figure 2B). The proportion of patients who underwent revascularization surgery showed a dosage-dependent pattern of the variant, being the highest in homozygotes (60% in AA, 34% in GA, and 16% in GG; P for trend <0.001). Seizure as the initial clinical manifestation was more common in homozygotes than in heterozygotes or those with the wild-type variant (40% vs. 3%, P=0.03; 40% vs. 3%, P=0.06; respectively). Homozygotes were more susceptible to PCA involvement than heterozygotes and wild-type (80% vs. 20%, P=0.02; 80% vs. 10%, P<0.01; respectively). PCA involvement showed a dose-dependent pattern of the variant, being the highest in homozygotes (80% in AA, 20% in GA, and 10% in GG; P for trend <0.001). The results of the subgroup analysis of genotype–phenotype correlations for RNF213 R4810K variant with the age at onset are described in the Supplementary Results, Supplementary Tables 2-4, and Supplementary Figure 3.
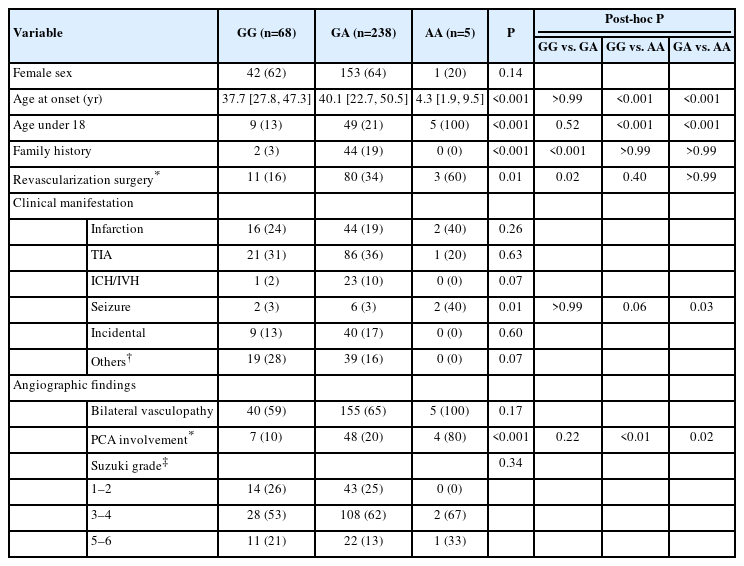
Correlation of clinical characteristics with the R4810K genotype of RNF213 in patients with moyamoya disease
Among 311 MMD patients, 293 with at least 3 months of follow-up were analyzed for the association between the RNF213 R4810K variant and long-term patient outcomes. During the median follow-up of 35 months after the diagnosis of MMD, 30 cases of cerebral infarction, 51 of TIA, 11 of ICH/IVH, and 2 deaths occurred (Supplementary Table 5). The risk of cerebral infarction after the diagnosis of MMD was approximately six times higher in homozygotes than in those with the wild-type variant (unadjusted hazard ratio, 6.38; 95% confidence interval 1.20–33.89; P=0.03) (Table 2). Among the 94 patients who underwent revascularization surgery, 99 hemispheres from 65 patients with MMD were included in this investigation (Supplementary Table 6). The increase in the caliber change ratios—defined as the ratio of postoperative caliber diameter to preoperative caliber diameter—for the superficial temporal artery was significantly higher in patients with the RNF213 R4810K variant (median 1.27, interquartle range [IQR] 1.12–1.42) than in those with the wild-type variant (median 1.12, IQR 1.01–1.23; P=0.046) (Figure 1).
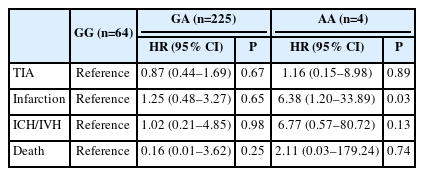
Correlation between clinical outcomes and the R4810K variant of RNF213

Association of postoperative collateral development and the RNF213 R4810K variant in moyamoya disease. The caliber change ratios for the superficial temporal artery were compared between patients with the RNF213 R4810K variant and those with the wild-type variant. RNF213, ring finger protein 213; GG, wild type; GA, heterozygote; AA, homozygote.
This study confirmed that the homozygous R4810K genotype is not only associated with an earlier onset of MMD, but also with seizures and PCA involvement. Previous studies have not demonstrated an association between the R4810K variant and seizures [3,4,6]. Additionally, the association between the R4810K variant and initial angiographic findings of MMD, such as bilaterality and PCA involvement, has not been fully established [3,4,8]. This is the most extensive study to assess the genotype–phenotype correlation of RNF213 R4810K variant in Korean patients. We clarified that the homozygous R4810K variant of RNF213 predicts the early onset of MMD and PCA involvement in Korean patients. Moreover, the R4810K variant was associated with seizures and influenced the clinical phenotype depending on the age at onset, indicating an extensive role of the RNF213 R4810K variant in MMD.
To our knowledge, this is the first study to demonstrate that the homozygous R4810K variant has a higher risk of future cerebral infarction than that of the wild-type, indicating that homozygotes are at high risk for later cerebral infarction, and more aggressive bypass surgery can be considered in these patients. Moreover, patients with the RNF213 R4810K variant showed better revascularization outcomes than those of patients with the wild-type variant, as reported in previous studies [8,9]. Although the precise pathophysiological role of RNF213 in MMD remains unclear, the present and previous studies’ results support its role in angiogenic function [2,10].
Our study had some limitations. Selection bias was unavoidable owing to its retrospective design. Only 8% of patients diagnosed with MMD underwent RNF213 genotyping, and few homozygous patients were included. Moreover, rare variants of the RNF213 gene were not analyzed.
In conclusion, the R4810K variant of RNF213 strongly correlated with an earlier age of onset, seizure at presentation, PCA involvement, future cerebral infarction, and better development of collaterals after bypass surgery in patients with MMD. Our study suggests a broader genotype–phenotype correlation than was previously assumed and provides informative data on the role of RNF213 in the clinical management of MMD.
Supplementary materials
Supplementary materials related to this article can be found online at https://doi.org/10.5853/jos.2023.00297.
Clinical and angiographic characteristics of patients with moyamoya disease
Genotype–phenotype correlation of the RNF213 R4810K variant in adult moyamoya disease
Genotype–phenotype correlation of the RNF213 R4810K variant in pediatric moyamoya disease
Comparison between pediatric and adult moyamoya disease among RNF213 R4810K heterozygotes
Clinical Outcomes in patients with moyamoya disease and the R4810K variant of RNF213
Characteristic of patients with revascularization surgery
Flowchart for the selection of moyamoya disease patients with ring finger protein 213 (RNF213) genotyping.
Age distribution patterns in moyamoya disease and correlation between ring finger protein 213 (RNF213) R4810K genotype and age at onset. (A) Dual peak distribution of moyamoya disease. (B) A box plot of the age at onset among 3 groups of patients: homozygotes (AA), heterozygotes (GA), and wild types (GG) of RNF213 R4810K variant.
Genotype–phenotype correlation of RNF213 R4810K variant in moyamoya disease. (A) All patients with moyamoya disease. (B) Patients with adult moyamoya disease. (C) Patients with pediatric moyamoya disease. RNF213, ring finger protein 213; GG, wild type; GA, heterozygote; AA, homozygote; FHx, family history; TIA, transient ischemic attack; ICH/IVH, intracranial cerebral hemorrhage/intraventricular hemorrhage; PCA, posterior cerebral artery.
Notes
Funding statement
None
Conflicts of interest
The authors have no financial conflicts of interest.
Author contribution
Conceptualization: TO, KYL. Study design: all authors. Methodology: TO, KYL. Data collection: TO. Investigation: TO, KYL.. Statistical analysis: TO, YHJ. Writing—original draft: TO. Writing—review & editing: all authors. Funding acquisition: KYL. Approval of final manuscript: all authors.